
Pulmonary edema is a condition of the respiratory system in which excessive fluid accumulates within the air sacs of the lungs. When the disease develops over a short period, it is termed Acute Pulmonary Edema. When it worsens slowly, it is called chronic pulmonary edema. Another variant known as “flash” pulmonary edema happens almost instantly after the occurrence of a precipitating event.
Symptoms
The most common symptom of acute pulmonary edema is a rapidly progressive shortness of breath. Whereas a healthy person may breathe heavily only with strenuous exercise, a patient with acute pulmonary edema may do so while performing routine daily activities, or even at rest.
Coughing up blood is another symptom of the disease. This usually means that the patient produces sputum tinged with blood, appearing pink in colour.
Patients may also experience a high-pitched whistling sound when they breathe. This “wheezing” is caused by a narrowing of the airways, which is also associated with this condition. Your physician may use a stethoscope to better identify this abnormal respiratory noise.
» Now, let’s discuss acute pulmonary edema causes.
Causes


Because of how deeply the heart and the lungs are intertwined, the causes of pulmonary edema are often related to an insult affecting the heart.
» To better understand these pathological entities, it helps to take a look at the relations between the heart, the lungs, and the blood vessels that connect them:
The human heart is composed of four chambers: Two small atria above, and two large ventricles below. The atria receive blood coming to the heart, and the ventricles pump blood away from the heart. The heart can thus be divided into two sides: Right and left. Hence, we have a right atrium, a right ventricle, a left atrium, and a left ventricle.
The right ventricle pumps blood to the lungs through the pulmonary artery. This blood travels through the pulmonary vascular tree and gets loaded with oxygen from the air sacs. The lungs, having performed their function of oxygenating the blood, pass this blood into the pulmonary veins, which are connected to the left atrium. The blood then ends up in the left ventricle, which pumps it to the rest of the body.
Regarding the mechanisms by which blood is pumped from the heart: An important structure that prevents the backflow of blood after pumping is the heart valve. Heart valves exist between atria and ventricles, and also between the heart and its great vessels: the aorta and the pulmonary artery. They close immediately after cardiac contraction, and re-open only to allow the blood flow to the correct direction.
With this in mind, how would a cardiac condition cause acute pulmonary edema? It often boils down to this: An abnormality of the heart impairs its ability to pump the blood it receives from the lungs. With each inefficient heartbeat, more and more blood accumulates in the left ventricle. The increased pressure is then transmitted to the left atrium above, then back into the pulmonary veins and pulmonary vasculature. The pulmonary vessels thus congested and with no method of relief begin to leak fluid into the air spaces. This makes it much more difficult for oxygen to enter the patient’s blood, thus impairing the main function of the lungs: Gas exchange.
Conditions that can cause this process include a heart attack (also called an acute myocardial infarction), which is often precipitated by decades of atherosclerosis, a condition which narrows the blood vessels of the body, often including those that supply the heart itself: The coronary arteries.
If the aforementioned heart valves fail to prevent the backflow of blood, blood will be regurgitated back into the left ventricle with each heartbeat. Examples of this include Mitral regurgitation and Aortic regurgitation. The mitral valve divides the left ventricle and the left atrium, and the aortic valve secures the largest blood vessel in the body: The aorta.
An abnormal cardiac rhythm may also compromise the orchestra of heart chamber contraction and relaxation, leading to a cacophony of uncoordinated heartbeats that end in acute pulmonary edema.
Renal artery stenosis

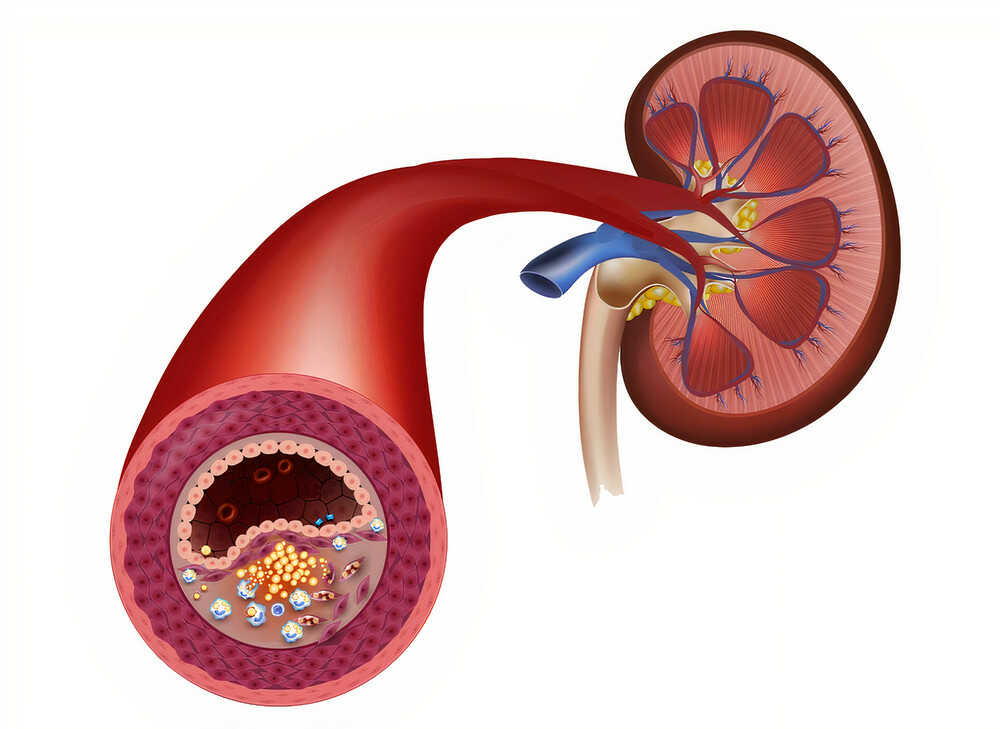
The kidneys are supplied by the renal arteries. These organs get rid of excessive or unneeded fluids and minerals by filtering the blood that they receive.
Atherosclerosis of the renal arteries, or a structural abnormality of their wall narrows the caliber of these vessels, which decreases the amount of blood going to the kidneys. The kidneys wrongly infer that the whole body must be suffering from a low blood volume, and they launch a cascade of chemicals that increase the blood volume, referred to as “RAAS” or the Renin Angiotensin Aldosterone System. This overwhelms the heart, causing back-up of blood into the lung’s vessels and the onset of acute pulmonary edema.
Treatment


Acute pulmonary edema is a dangerous condition that warrants rapid hospitalization and treatment. Before correcting the precipitating factors, resuscitative steps must be undertaken quickly. The primary step is to secure an open, clear airway. This may be achieved by simply encouraging the patient to cough, or may require the physician to perform a maneuver such as the Heimlich maneuver.
The second step is to administer oxygen, which restores the normal oxygen saturation of the blood. This is usually given by face mask or nasal prongs.
The third step is to administer drugs to decrease the load on the heart. These medications achieve the desired outcome through a variety of mechanisms. Diuretics increase the volume of urine, siphoning excess fluid from the circulation. Angiotensin Converting Enzyme Inhibitors (ACE inhibitors) and Angiotensin II Receptor Blockers (ARBs) halt the RAAS system of the kidneys, preventing them from increasing the blood volume to the detriment of cardiac function.
After the patient is stabilized, attention should be shifted towards the cause of the acute pulmonary edema. Each condition requires a specific treatment, which may be medical or surgical. For example, patients with incompetent heart valves may need a heart valve replacement operation. People with arrhythmia need to be maintained on anti-arrhythmic medication. Someone with an acute myocardial infarction would need thrombolytics or a PCI (Percutaneous Coronary Intervention), followed by antiplatelet and anticoagulant drugs.