

The liver is one of the most active and vital organs of your body. The large organ covers up a lot of space in your abdominal region. Therefore, the liver is entitled to many duties that are crucial for the optimal working of the body.
There is a long list of functions performed by the liver:
-
- Produces bile to enhance digestion of fats in the small intestine
- Produces cholesterol that carries fats (throughout the body)
- Converts and stores excess glucose to glycogen
- Stores excess iron
- Regulates amino acid levels and blood clotting factors
- Enhances the immune system
- Clears the body of poisons, drugs, ammonia, etc.
These are the most evident but not the only activities performed by the dark red organ. For example, a small hepatitis B virus (HBV) can cause damage and inflammation despite its large size.
“Hepatitis” means inflammation of the liver, and when the hepatitis B virus causes it, the disease is known as Hepatitis B. It is a chronic liver disease that is pretty common in underdeveloped and developed countries. However, chronic ailment is highly endemic in low-income countries due to limited resources and medical facilities.
According to the World Health Organization, as of 2019, there were 296 million people (estimated value) living with chronic hepatitis B infection. The counter for new patients annually was 1.5 million. The approximate number of deaths due to hepatitis B is 620,000 per year.
It exists in two forms, i.e., acute and chronic. Acute infections acquired by infants develop into a common form in most cases. The progression of chronic hepatitis B is slow, and the symptoms are not noticeable.
Liver cirrhosis is a likely outcome of chronic hepatitis B. According to a study, 40% of men who acquire hepatitis B perinatally die of cirrhosis. The percentage is smaller for women, i.e., 15%.
Hepatitis B Causes
Entry of the hepatitis B virus is a must for you to get infected. Hepatitis B virus is acquired when one comes into contact with an infected person. The transmission of HBV is worth discussing. There are several ways by which you can become infected by HBV, which are discussed below:
Transmission
Hepatitis B is a contagious disease that travels via the blood, semen, or other blood fluids. The most common ways of transmission include:
-
- Perinatal transmission (mother to child)
- Direct blood contact with infected person’s blood (blood transfusions)
- Using contaminated needles
- Having intimacy or sex (vaginal, anal, etc.) with HBV infected person
- Sharing personal items such as razors, blades, etc. with hepatitis B patient
Though the virus also resides inside the saliva, there is no transmission through shared utensils or even kissing. The most common transmission route is perinatal, i.e., from mother to child during the process of childbirth. As per a study, viral transmission occurs only in women having a high viral load. Transplacental leakage of maternal blood may also be the culprit in transmitting the virus from the mother to the fetus. However, this route is the most common one.
Risk Factors
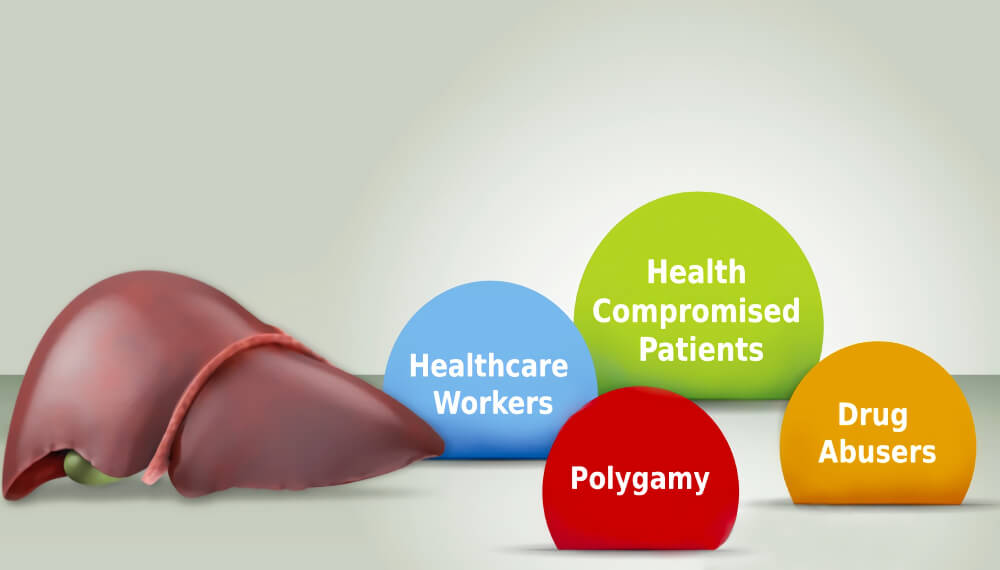

Based on the modes of transmission, certain social groups are at a higher risk of acquiring the disease. High-risk groups include:
1) Healthcare Workers
Doctors, dentists, and paramedical staff are at significant risk of acquiring hepatitis B from a patient. HBV is highly transmissible, and healthcare providers dealing with mucous membranes (dentists) and parenteral membranes have reported transmission from patients.
2) Polygamy
Men and women having multiple sex partners are a step closer to acquiring and further transmitting HBV.
3) Drug Abusers
Drug abusers usually share hypodermic needles. If one of them is infected, sharing the blood-contaminated needles can be a source of transmission.
4) Health Compromised Patients
People suffering from chronic liver and kidney disease are prone to developing hepatitis B. Old diabetics have weak immune systems that increase their chances of falling prey to hepatitis B.
Symptoms
There is no hard and fast rule regarding the appearance of symptoms. Acute hepatitis B symptoms may not appear for weeks or even months. Chronic hepatitis’ onset is also slow. In both cases, the following symptoms are observed:
1) Loss Of Appetite


Abruptions in appetite is usually the primary manifestations of liver disease. Hepatitis patients typically complain of loss of appetite as an initial symptom. A study published in the Journal of Viral Hepatitis noted that hepatitis B patients showed two evident signs before being diagnosed with hepatitis B. The two most common symptoms reported include loss of appetite and fatigue. A whopping 79% of patients suffered from a loss of appetite, while the percentage of patients experiencing fatigue and energy loss was 90%.
In another study, pregnant women suffering from acute hepatitis B also reported a loss of appetite.
Many people complain of having the same desire to eat as they used to, while others claim to have no feeling of hunger. This is also accompanied by unintentional weight loss. One of the significant roles played by the liver is an enhancement in food digestion. Therefore, the suboptimal performance of the liver leads to poor digestion and thus weight loss.
Patients suffering from viral hepatitis infections might also experience alterations in taste sensations, further adding to abstinence from consuming food. This phenomenon, combined with a decreased urge to eat, leads to rapid weight loss and fatigue.
2) Fatigue And Weakness


Chronic liver disease has a direct impact on the patient’s energy levels. There are many chronic liver diseases, including hepatitis (A, B, C, etc.), hepatocellular carcinoma, etc.
Lack of energy or fatigue is a commonly faced problem by chronic hepatitis B patients. Conversely, fatigue and fever might be the initial symptoms of hepatitis B infection.
The ailment takes a direct toll on your body’s energy levels, thereby leaving you deficient in it. In addition, a link between fatigue and hepatitis B was found in a study carried out in 2018.
Chronic fatigue is a possible side effect of hepatitis B. However, the extent of fatigue and reduced quality of life (due to fatigue) is subject to independent factors. Patients who exercise regularly experience lower fatigue levels than those who spend a sedentary life.
3) Joint/Muscle Aches


Muscle and joint ache may not be present in all patients but is a feature of hepatitis B. Once inflammation takes over the liver, there can be multiple manifestations of a diseased organ. One of these presentations is a muscle and joint pains.
There have been multiple case reports in which patients have presented with joint and muscle pains before being diagnosed with acute hepatitis B. For example, a 28-year-old woman reported having severe pain in the shoulder, elbow, and hand joints (metacarpophalangeal, proximal interphalangeal joints).
A 35-year-old man presented with a painful and stiff neck and upper and lower back joints without any evident reason. There were no other symptoms. However, serum AST was raised. HBsantigen test came out positive after seven weeks. This indicated the presence of HBV in the body that caused the aches.
A 30-year-old heroin addict was hospitalized for severe pain. The patient did not have any hepatic symptoms initially; however, he became jaundiced and had raised levels of bilirubin and alkaline phosphatase after 40 days. In this particular case, joint pain was the initial presenting symptom of hepatitis B infection.
Patients with acute hepatitis B often suffer from arthralgias (joint pains) and myalgias (muscle pains). In an old study, eighteen patients with acute hepatitis presented with arthritis and arthralgias. Acute hepatitis B can cause severe muscle and joint pain. This discomfort can be picked up well before other symptoms of the ailment start to appear.
Research suggests rheumatological manifestations (arthralgias and myalgias) are found in patients with hypothyroidism, rheumatoid arthritis, and viral hepatitis (B and C).
4) Jaundice

Jaundice is a condition in which the skin and mucous membranes turn yellow. A doctor diagnoses jaundice by observing the white of the eyes of the patient. This is because the eyes also change color due to the high bilirubin levels in the body.
This was the most prominent manifestation that led to the discovery of the hepatitis B virus. Infestation of hepatitis virus leads to the breakdown of blood cells. Hyperbilirubinemia (excessive bilirubin in the blood) is a medical condition that leads to jaundice.
Old red blood cells are broken down into bilirubin in the spleen. This bilirubin is then transferred to the liver, which creates bile. If the liver (due to hepatitis B virus infection) can not utilize the bilirubins, they get accumulated in the blood. Here the yellow bilirubin imparts its color, thereby making the skin and eyes yellow.
Jaundice can result from several conditions, including drug abuse and infection. However, this is most frequently the result of underlying viral hepatitis infection. According to a study conducted in Kenya, jaundice is most commonly associated with viral hepatitis, specifically chronic HBV infections.
At least 30% of hepatitis B patients develop jaundice. In addition, as per a study, pregnant hepatitis B patients have higher bilirubin levels in the body and more evident jaundice than non-pregnant patients.
5) Vasculitis


Inflammation of the blood vessels is known as vasculitis. In addition, patients suffering from hepatitis B face a disease called polyarteritis nodosa. The rare disorders lead to inflammation of the vessels that in turn cause organ damage.
Hepatitis B-induced Polyarteritis nodosa may present itself in the following ways:
- Abdominal pain
- Bloody stools
- Painful and sore muscles
- Skin ulcers
Studies have found a strong link between polyarteritis nodosa and hepatitis B infection. Moreover, as per research, polyarteritis nodosa (PAN) can give rise to renal and gastrointestinal complications, which can be fatal.
6) Abdominal Pain/Discomfort


The liver covers a large amount of your abdominal region. When the liver diseases, it can indicate it by causing pain. In most cases, liver pain is a dull ache that may come with a throb. The pain is generally localized to the upper right abdomen. Some people might mistake it for heart pain as it may become stabbing in nature; however, right-sided pain indicates liver involvement.
The excruciating pain can also radiate to the right shoulder blade and interfere with your breathing. Hepatitis is known to cause liver pain.
7) Nausea And Vomiting

Nausea and vomiting are the effects of a myriad of underlying conditions. From heart attack to kidney disease, nausea and vomiting are common to plenty of health problems. Liver maladies can also initiate nauseated feeling or induce vomiting. When paired with hepatic symptoms, these symptoms can help reach a diagnosis.
A darker than normal colored urine should also ring bells as they may be a presenting feature of underlying viral hepatitis.
Diagnosis

Diagnosing hepatitis B requires a series of laboratory tests. On the presence of the symptoms mentioned above, your doctor will recommend you some blood tests that are discussed below:
A) Liver Function Tests (LFTs)
The most basic test carried out to investigate the performance of the liver is the liver function test. It comprises different liver enzymes that indicate infectious conditions. These tests reflect the liver damage and do not specify the disease itself.
In cases of acute hepatitis B, serum alanine transaminase (ALT) levels are raised that are correlated with the clinical picture (jaundice in most cases). In addition, Aspartate aminotransferase (AST) also helps monitor potential liver damage caused by hepatitis B.
Alpha-Fetoprotein (AFP) raised levels point towards presence of hepatocellular (liver) cancer. As hepatitis is the leading cause of liver cancer, values of AFP are critical.
B) Hepatitis B Tests
To reach a definitive diagnosis, your doctor will recommend you to get the hepatitis panel test which includes the following tests:
1- Hepatitis B Surface Antigen Test (HbsAg)
If infected with HBV, the result will show “positive” or “reactive.” This particular test looks for the surface antigens of the hepatitis B virus in the blood. After the result is positive, the search for acute or chronic type starts. Research suggests HBsAg is a rapid diagnostic test for Hepatitis B infection.
A 2017 study claims HBsAg to have excellent specificity and good sensitivity in diagnosing hepatitis B infection.
2- Hepatitis B Core Antigen Test
The core antigen test shows the current state of infection. For example, it comes out positive if you have acute or chronic hepatitis B infection.
3- Hepatitis B Surface Antibody (Anti-HBs/HBsAb)
This test detects the presence of antibodies (from the body) against the viral antigen. In addition, the test indicates the immune status of the patient. If Anti-HBs is positive, the patient has developed antibodies and is immune.
4- Hepatitis B Core Antibody (Anti-HBc/HBcAb)
A positive/reactive test means a current hepatitis B infection. The test results are fully understood by correlating the results of other tests.
C) Liver Tests
Some more tests will be recommended to check for extensive liver damage. These include liver ultrasound and liver biopsy.
Treatment And Prognosis


The treatment strategies differ for acute and chronic hepatitis B infection. An episode of acute hepatitis B infection goes away on its own and does not need any medical treatment. However, chronic hepatitis B has to be dealt with pharmacological intervention.
The following modalities are available to treat chronic hepatitis:
1) Antiviral Drugs
The first line of treatment against the activity of the virus is antiviral drugs. A wide variety of antiviral drugs available have proven to be of benefit in the fight against HBV. most commonly used drugs include:
-
- Adefovir
- Lamivudine
- Tenofovir
- Entecavir
- Telbivudine
It was found in a study that the same dosage of tenofovir (300 mg) had better antiviral effects as compared to adefovir through a 48-week administration program.
A study demonstrated that lamivudine has an excellent safety profile and effectively manages patients with chronic hepatitis B.
Modern Research
Doctors and researchers are now creating better ways to deal with chronic hepatitis B patients. For example, as per a meta-analysis, it is completely safe and effective to administer prophylactic antiviral therapy to pregnant mothers to prevent mother-to-child transmission of the hepatitis B virus.
Antiviral therapy has the potential to improve symptoms and reduce viral load in patients. This therapy, paired with immune response boosts, can become more effective in the future.
Research is ongoing to discover new classes of effective and safe antiviral drugs. In addition, new direct-acting antivirals are under development that includes entry inhibitors, cccDNA targeting, and HBsAg secretion inhibitors.
It was revealed in a 2020 study HBsAg level in the body nosedived after direct-acting antiviral therapy. So the newer class of drugs can be pretty effective for prophylaxis and management of HBV/HCV co-infected patients as well.
2) Antibody Injections
Antibodies are the body’s natural cells produced in response to a viral antigen. However, man-made synthetic versions of antibodies are available that can be injected to fight infection. For example, Interferon alpha-2b is a commonly used interferon to treat chronic hepatitis B infection.
Different genotypes of patients having hepatitis B have different responses to interferon therapy. It has been observed that HBV genotype B has a better response to interferon-alpha therapy. Older studies found interferon therapy and Polyethylene Glycol (PEG)- Interferon therapy (IFN) to have the only average antiviral capacity and have some evident side effects.
However, a study claimed IFN-alpha to be therapeutically effective due to its potent antiviral and immunomodulatory properties. Furthermore, long-term analysis of alpha-interferon treatment revealed that the therapy leads to remission of the virus and improvements in liver structure (histology).
Modern Research
According to modern research, interferon-alpha has evident anti-viral properties, but this function is compromised in the presence of HBV. This effect is due to the interaction between IFN stimulated genes (ISG) and HBV proteins. Thus, small molecules must be designed that interfere with this communication and enhance the efficacy of therapy.
According to a new switch study, chronic hepatitis B patients can attain evident HbsAg loss by switching to PEG-IFN-alpha-2a therapy.
In addition to interferon therapy (PEG-IFN), neucleot(s)ide analogs (NUCs) are also utilized to decrease the viral load further. The best antiviral drugs used in combination with NUCs include:
-
- Tenofovir disoproxil fumarate
- Tenofovir alafenamide
- Entecavir
Interferon therapy can have some side effects. However, using it with NUCs has better results in hepatitis B patients.
3) Liver Transplant
A liver transplant is the only option left if the virus has extensively damaged the organ. It is well-documented that a liver transplant is the only option when the following changes have occurred:
-
- There are severe acute hepatitis flares
- Decompensated cirrhosis of the liver has taken place
- Hepatitis B has converted into hepatocellular carcinoma
Lifelong antiviral therapy is recommended after liver transplantation. This is because recurrent hepatitis infection can significantly impair graft and compromise patient survival.
Prevention

Hepatitis B infection can be prevented thanks to the creation of vaccines. According to the World Health Organization, the Hepatitis B vaccine offers 98-100% protection against hepatitis B infection. There are different ways vaccines induce the development of the body’s immune response towards a viral agent.
Some vaccines use dead microorganisms, while some inject attenuated viruses into the body. Only viral antigens and not the whole virus are used to trigger an immune response. All these processes have the same result, i.e., immune cells (antibodies) production against infectious agents.
There are 2-dose and 3-dose hepatitis B vaccines available. However, studies suggest that a two-dose vaccine (recombinant hepatitis B vaccine) is better than a three-dose vaccine.
Conclusion


Inflammation of the liver by hepatitis B virus (HBV) is termed hepatitis B. It is contagious and is transmitted via the exchange of body fluids. The virus is most commonly transmitted to infants via the mother-to-child route. However, people committing polygamy sharing personal items and needles are at a greater risk of developing hepatitis B.
The disease manifests itself as hepatic and extrahepatic symptoms. Hepatic symptoms include abdominal pain, loss of appetite, weight changes, and jaundice. Extrahepatic symptoms include muscle/joint aches, fever, dark urine, vasculitis, and fatigue. Hepatitis B is diagnosed via blood tests (CBC, LFTs) and hepatitis serology tests (HbsAg, Anti-Hbs. Anti-Hbc, etc.).
Acute hepatitis B doesn’t need any treatment, while antiviral medicines such as lamivudine, tenofovir, etc. are used to combat the virus. Interferon injections and nucleoside analogs are also used in the treatment. Hepatitis B vaccine is 98-100% effective against infection.
References
-
- Zampino, Rosa, et al. “Hepatitis B virus burden in developing countries.” World journal of gastroenterology42 (2015): 11941.
- Trépo, Christian, Henry LY Chan, and Anna Lok. “Hepatitis B virus infection.” The Lancet9959 (2014): 2053-2063.
- Wiseman, Elke, et al. “Perinatal transmission of hepatitis B virus: an Australian experience.” Medical Journal of Australia9 (2009): 489-492.
- Xu, De‐Zhong, et al. “Risk factors and mechanism of transplacental transmission of hepatitis B virus: a case‐control study.” Journal of medical virology1 (2002): 20-26.
- Lewis, Jessica D., Kyle B. Enfield, and Costi D. Sifri. “Hepatitis B in healthcare workers: Transmission events and guidance for management.” World journal of hepatology3 (2015): 488.
- Hann, H‐W., et al. “Symptomatology and health attitudes of chronic hepatitis B patients in the USA.” Journal of viral hepatitis1 (2008): 42-51.
- Han, Yong-Tao, et al. “Clinical features and outcome of acute hepatitis B in pregnancy.” BMC infectious diseases1 (2014): 1-7.
- Jang, Yeonsoo, Sunjoo Boo, and Hyera Yoo. “Hepatitis B virus infection: Fatigue-Associated illness experiences among Koreans.” Gastroenterology Nursing5 (2018): 388-395.
- Zhong, Chunxiu, et al. “Risk factors associated with fatigue in chronic hepatitis B patients.” Patient preference and adherence13 (2019): 1065.
- Alpert, Elliot, Kurt J. Isselbacher, and Peter H. Schur. “The pathogenesis of arthritis associated with viral hepatitis: complement-component studies.” New England Journal of Medicine4 (1971): 185-189.
- Oliveira, Ídila Mont’Alverne Xavier de, and Rita do Socorro Uchôa da Silva. “Rheumatological manifestations associated with viral hepatitis B or C.” Revista da Sociedade Brasileira de Medicina Tropical52 (2019).
- Block, Timothy M., et al. “A historical perspective on the discovery and elucidation of the hepatitis B virus.” Antiviral research131 (2016): 109-123.
- Han, Yong-Tao, et al. “Clinical features and outcome of acute hepatitis B in pregnancy.” BMC infectious diseases1 (2014): 1-7.
- Ochwoto, Missiani, et al. “Hepatitis B infection is highly prevalent among patients presenting with jaundice in Kenya.” BMC infectious diseases1 (2016): 1-14.
- Guillevin, Loïc, et al. “Polyarteritis nodosa related to hepatitis B virus. A prospective study with long-term observation of 41 patients.” Medicine5 (1995): 238-253.
- Guillevin, Loïc, et al. “Hepatitis B virus-associated polyarteritis nodosa: clinical characteristics, outcome, and impact of treatment in 115 patients.” Medicine5 (2005): 313-322.
- Wilkins, Thad, Richard Sams, and Mary Carpenter. “Hepatitis B: screening, prevention, diagnosis, and treatment.” American family physician5 (2019): 314-323.
- Franzeck, Fabian C., et al. “Viral hepatitis and rapid diagnostic test based screening for HBsAg in HIV-infected patients in rural Tanzania.” PLoS One3 (2013): e58468.
- Amini, Ali, et al. “Diagnostic accuracy of tests to detect hepatitis B surface antigen: a systematic review of the literature and meta-analysis.” BMC infectious diseases1 (2017): 19-37.
- Zoulim, Fabien, and Robert Perrillo. “Hepatitis B: reflections on the current approach to antiviral therapy.” Journal of hepatology48 (2008): S2-S19.
- Marcellin, Patrick, et al. “Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B.” New England Journal of Medicine23 (2008): 2442-2455.
- Lok, Anna SF, et al. “Long-term safety of lamivudine treatment in patients with chronic hepatitis B.” Gastroenterology6 (2003): 1714-1722.
- Funk, Anna L., et al. “Efficacy and safety of antiviral prophylaxis during pregnancy to prevent mother-to-child transmission of hepatitis B virus: a systematic review and meta-analysis.” The Lancet Infectious Diseases1 (2021): 70-84.
- Rehermann, Barbara, and Robert Thimme. “Insights from antiviral therapy into immune responses to hepatitis B and C virus infection.” Gastroenterology2 (2019): 369-383.
- Asselah, Tarik, et al. “Targets and future direct-acting antiviral approaches to achieve hepatitis B virus cure.” The Lancet Gastroenterology & Hepatology11 (2019): 883-892.
- Yeh, Ming-Lun, et al. “Hepatitis B-related outcomes following direct-acting antiviral therapy in Taiwanese patients with chronic HBV/HCV co-infection.” Journal of hepatology1 (2020): 62-71.
- Kao, Jia-Horng, et al. “Hepatitis B genotypes and the response to interferon therapy.” Journal of hepatology6 (2000): 998-1002.
- Rijckborst, Vincent, and Harry LA Janssen. “The role of interferon in hepatitis B therapy.” Current hepatitis reports4 (2010): 231-238.
- Robek, Michael D., Bryan S. Boyd, and Francis V. Chisari. “Lambda interferon inhibits hepatitis B and C virus replication.” Journal of virology6 (2005): 3851-3854.
- van Zonneveld, Monika, et al. “Long‐term follow‐up of alpha‐interferon treatment of patients with chronic hepatitis B.” Hepatology3 (2004): 804-810.
- Tan, Guangyun, et al. “When hepatitis B virus meets interferons.” Frontiers in microbiology9 (2018): 1611.
- Hu, Peng, et al. “HBsAg loss with Peg-interferon Alfa-2a in hepatitis B patients with partial response to nucleos (t) ide analog: new switch study.” Journal of clinical and translational hepatology1 (2018): 25.
- Viganò, Mauro, et al. “Treatment of hepatitis B: Is there still a role for interferon?.” Liver International38 (2018): 79-83.
- Fung, James. “Management of chronic hepatitis B before and after liver transplantation.” World journal of hepatology10 (2015): 1421.
- Snydman, David R., Bruce Y. Tung, and Kris V. Kowdley. “Hepatitis B and liver transplantation.” Clinical infectious diseases10 (2005): 1461-1466.