

The Human Immunodeficiency Virus, more commonly known as HIV, is a virus that severely affects the body’s entire immune apparatus. Weakened by HIV, the host’s immune system becomes increasingly susceptible to infections and diseases and the Acquired Immune Deficiency Syndrome, more commonly known as AIDS, develops.
In other words, the condition known as AIDS refers to a broad spectrum of symptoms and conditions that appears due to a severe shortfall of the immune system caused by an acquired viral infection.
Once HIV infection occurs, the viral antibodies can take upwards of 3 to 4 weeks before reaching detectable levels. As such, during this time, known as the “window period,” laboratory tests can potentially give a negative result even if the patient has already become infected.
Therefore, while infection with HIV does not necessarily entail the development of AIDS, every person who has developed AIDS is invariably HIV positive. Furthermore, HIV infection develops across various stages, each identified by a set of distinct symptoms and other clinical indicators. Furthermore, most of the symptoms associated with HIV infection occur primarily well into the evolution of the infection and the appearance of AIDS.
Below we take a closer look at the most common symptoms:
1. Oral Disease

HIV weakens your immune system, making you vulnerable to a vast number of diseases. In fact, oral diseases as a direct result of infection are particularly common in HIV patients.
One of the most common oral manifestations of HIV is the appearance of oral warts. These warts can appear anywhere in the oral mucosa. Such warts, which are generally not painful, are caused by the Human Papilloma Virus, which is significantly more common in HIV positive patients than the rest of the population.
Another common oral complication for HIV patients is Hairy Leukoplakia. This condition is characterized by the appearance of whitish spots of with a “hairy” aspect on the tongue. These patches, which cannot be easily removed with a toothbrush, are benign and painless; however, because they only appear in people with weakened immune systems, they are often one of the first signs of HIV infection.
Painful canker sores on the lips, inside of the mouth, and tongue are also fairly common in patients with HIV infection.
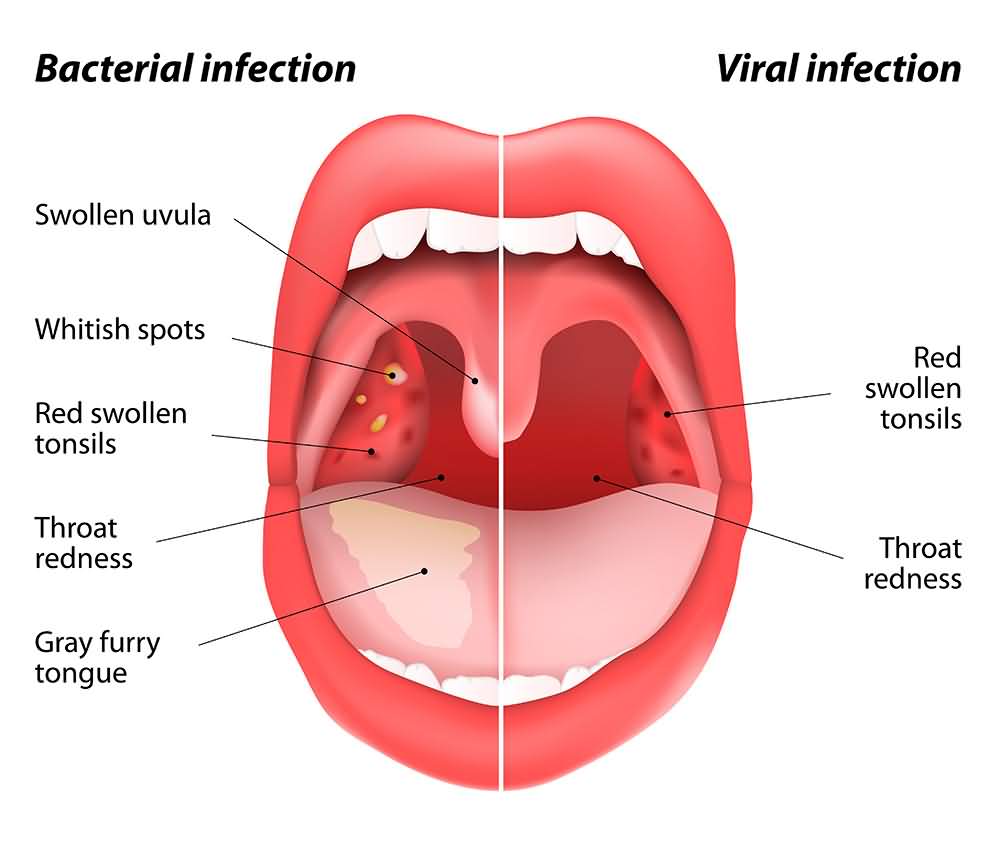
2. Pharyngitis

During the initial stages of infection, HIV reproduces exceptionally quickly and thus manifests with a very similar clinical picture to other more common viral infections such as the flu. As such, sore throats are relatively common in patients during the initial stages of HIV infection.
Just like in other, more benign infections, the throat or pharynx becomes inflamed. This inflammation causes pain and significant discomfort when talking or swallowing.
3. Fungal Infections

HIV patients are very prone to suffer from opportunistic infections due to the ever-decreasing cell-mediated immune function. One such condition is Candidiasis, a fungal infection caused by a strain of yeast called Candida.
Candidiasis of the mouth is probably one of the most common manifestations in HIV patients and Candidiasis of the esophagus is one of the defining signs of AIDS. However, HIV patients also commonly experience candidiasis infections of the skin and, in the case of females, the vagina.
Symptoms and signs of Candidiasis of the mouth and throat include whitish plaques on the inside of the mouth, pain, and an altered sense of taste. Candidiasis of the esophagus can cause sore throat and difficulty when swallowing and in some cases, it may cause pain along the upper chest. Vaginal Candidiasis is characterized by white discharge and a pervasive itching or burning sensation.
Other common fungal infections in HIV patients include Pneumocystosis, Cryptococcosis, Histoplasmosis), and Talaromycosis.
4. Chronic Pelvic Inflammatory Disease


Pelvic inflammatory disease, or PID, is an umbrella term for a distinct set of conditions and clinical manifestations that affect women suffering from an inflammatory disorder of the genital tract. These conditions include endometritis, salpingitis, salpingooforitis, fallopian tube abscesses, pelvic peritonitis and in extreme cases, septic shock.
Pelvic inflammatory disease is generally the result of an infection caused by common bacteria or virus. However, PID is commonly seen in females with HIV infection. The most commonly reported symptoms include lower abdominal pain, vaginal discharge, irregular menstruation, and painful intercourse.
PID can cause serious complications, including infertility and, if left untreated, death.
5. Fatigue


Asthenia is one of the most common symptoms of patients with HIV infection and AIDS.
This pervasive sense of physical fatigue is particularly troubling because it has the potential to result in a crippling disability, which could make even the simplest of mundane tasks exceedingly tricky to perform. For example, patients with severe asthenia are unable to climb stairs or even complete household chores.
HIV-related asthenia may be caused by a variety of factors such as antiretroviral medications, lack of sleep, poor diet, stress, and depression. However, no direct, consistent correlation has been found between asthenia and HIV infection.
Unfortunately, many in the medical community view asthenia as an inevitable manifestation, and thus, very little research has been done on the subject.
6. Sudden Weight Loss


The progression of HIV infection often involves a drastic loss of body weight.
Several factors contribute to HIV-related weight loss:
For example, low appetite is a common side effect of advanced HIV infection. Additionally, many of the drugs and medications that are prescribed to HIV/AIDS patients can dramatically alter a patients sense of appetite and satiety. When this is compounded by the various oral diseases that commonly plague HIV patients, the result is a dramatically diminished ingestion of food and a subsequent loss of weight.
Additionally, the basal metabolic rate of HIV patients tends to increase overall as the body uses more and more energy to fight off the growing viral load. Furthermore, HIV patients are prone to various infections and conditions that can potentially interfere with nutrient absorption along the gastrointestinal tract; which can often result in diarrhea, a severe caloric deficit, and weight loss.
Unfortunately, these factors often create a vicious cycle where HIV infection increases caloric demand, while at the same time generating conditions which alter and decrease a patients’ ability to meet these increased metabolic requirements.
7. Bruising

Bruises are generally formed when the blood vessels that lie under the skin rupture, most often due to a blow or fall. Blood seeps out into the surrounding tissues and causes the characteristic bluish-black color. As bruises heal, typically within 2 to 4 weeks, they change color from purplish black to reddish-blue to yellowish-green.
The vast majority of bruises do not represent a medical concern as they disappear on their own without the need for treatment. However, some bruises which appear to be unrelated to any physical trauma or are larger than normal can, in fact, be considered a sign of latent HIV infection.
HIV related bruising is thought to be the result of a diminishing platelet count which invariably reduces the body’s clotting capacity.
8. Diarrhea

Diarrhea is easily the most commonly observed of all gastrointestinal symptoms in patients suffering from HIV infection.
Diarrhea can appear as a consequence of infection by an opportunistic infectious agent, as well as a side effect of antiretroviral medication.
In healthy individuals, diarrhea may last a few days, but in patients with advanced HIV infection, it is common to see chronic cases of diarrhea which persists for several weeks or months.
In some cases, diarrhea can be so severe that the patient easily eliminates several gallons of fluid per day. Diarrhea may be accompanied by abdominal pain, nausea, vomiting, weakness, and fever.
It is important to note that the most common infectious organisms responsible for diarrhea in patients with HIV are Cytomegalovirus, Cryptosporidium, and Giardia. These microorganisms can infect and cause diarrhea in healthy individuals as well, but in the case of HIV patients, the resulting diarrhea is almost invariably of a chronic nature.
9. Swollen Lymph Nodes
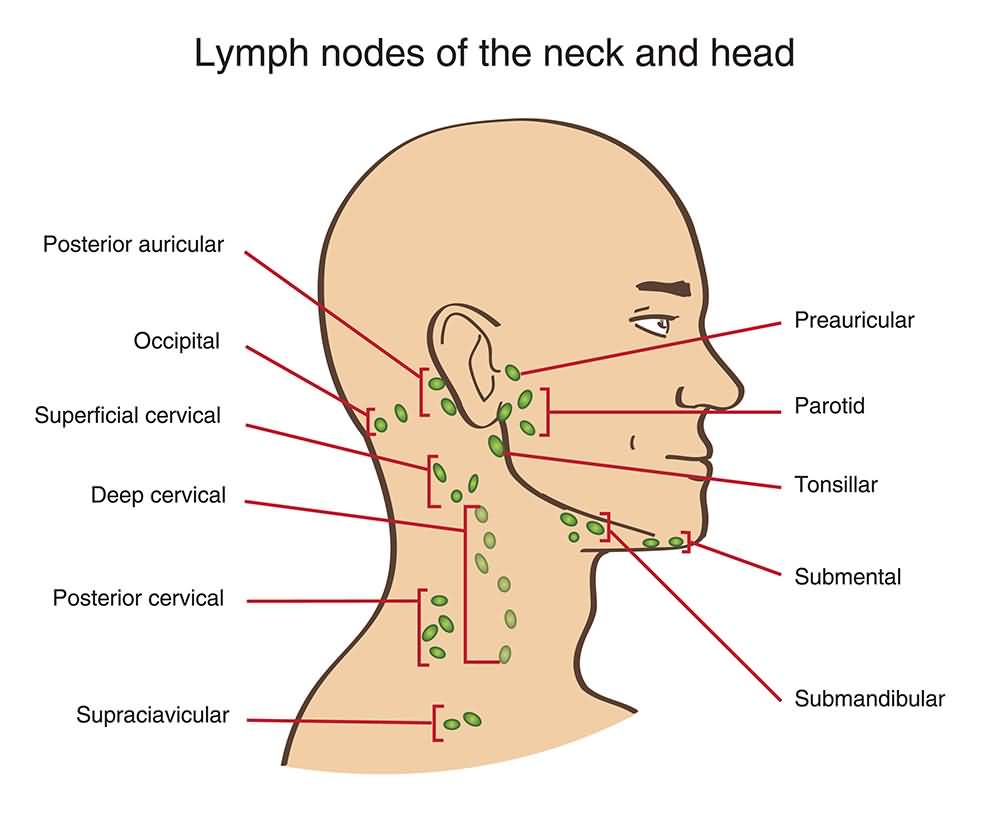

The human body is armed with a network of small, interconnected structures whose purpose is to hold B and T lymphocytes and help the body fight off infection. These structures, called lymph nodes, are found throughout the body, but they are mainly located in the neck, armpits, and groin.
If microorganisms such as bacteria or viruses enter the bloodstream, the lymph nodes become inflamed. In the case of HIV infections, close to 70% of patients who have tested positive for the virus report moderate to severe inflammation of the lymph nodes.
10. Dry Cough

The sudden appearance of a dry cough which does not produce phlegm can be a sign of early HIV infection or late-stage AIDS.
In the case of early infection, most patients report experiencing flu-like symptoms such as fever, headache, and a dry cough. However, in patients with late-stage AIDS, a persistent dry cough represents a grave danger and a potential risk of death, as often it can be a sign of Pneumocystis, a severe respiratory infection caused by a yeast-like fungus called Pneumocystis Jirovecii.
11. Kaposi’s Sarcoma


Kaposi’s sarcoma is a type of cancer that causes an overgrowth of blood vessels and manifests as small tumors or lesions on the skin. Although it is possible for HIV-negative patients to develop this condition, Kaposi’s Sarcoma has been associated with HIV/AIDS since the beginning of the epidemic.
The appearance of Kaposi’s tumors can be highly variable, with some patients experiencing minimal localized growth, and some experiencing a widespread and rapid emergence of lesions.
Kaposi’s Sarcoma in AIDS patients is associated with a herpes virus called Human Herpesvirus 8 or VHH-8. Currently, Kaposi’s Sarcoma is not curable, although in some cases the progress of the disease can be halted through the application of antiretroviral therapies.
12. Necrotizing Ulcerative Gingivitis

Bleeding from the gums is also commonly observed in patients with HIV. Often, the patient is suffering from necrotizing ulcerative gingivitis. This condition, which is an inflammatory gingival infection, is rapidly destructive and possesses a complex etiology.
Clinically it is characterized by necrotic ulcers of the interdental papilla, profuse and spontaneous bleeding and significant pain and discomfort. Patients suffering from necrotizing ulcerative gingivitis typically develop severe halitosis and lymphadenopathy.
Necrotizing ulcerative gingivitis can be a precursor to periodontitis; therefore, the prevention and treatment of high-risk individuals, such as people infected with HIV, can prevent the destruction of periodontal tissue.
13. HIV Associated Sensory Neuropathy

HIV Associated Sensory Neuropathy is a distal symmetric polyneuropathy and one of the most frequent neurological complications that affect patients infected with HIV. This painful condition affects up to 70% of HIV patients. Anywhere between 40% to 90% of patients report a painful burning, itching, or tingling sensation in the hands and feet.
This condition is directly associated with a significantly diminished quality of life, less independence in day to day life, and a higher prevalence of depression.
Treatment of HIV


HIV is a virus that essentially depresses humans’ immune system considerably enough to cause death from infections that can otherwise be easily resisted by their healthy counterparts. Since we treat humans as a whole and not as an organ, the treatment of HIV is complex. It is targeted at both the virus and the syndrome it causes (AIDS), as well as the infections that result from this infection. It should also be known that AIDS is the end stage of HIV infection that develops years after the infection is established.
To prevent the immune system from deteriorating to that level, the recommended regimen now in use is called HAART (Highly Active Antiretroviral Therapy). This regimen aims to increase the number of T-lymphocytes, which is indicated by what is termed CD4 count. T-lymphocytes are the body’s primary defense against many infections and cancers and are the basis of “Cell-mediated immunity.” Studies have also shown that successful HAART therapy decreased the risk of opportunistic infections and improved the overall psychiatric and renal health of patients with HIV. Current antiviral agents reduce the viral load to a number that allows the immune system to recover. Still, it doesn’t completely eradicate HIV from the body as per the date of writing this article.
Since the introduction of HAART therapy, the life expectancy and overall quality of life of HIV patients have significantly improved.
According to recent guidelines regarding primary care of HIV patients, the following has changed:
- HIV patients are now allowed to be vaccinated against infections as varicella and influenza, which was considered contraindicated before. This is because of the risk of the viruses used in the manufacture of such vaccines turning infective due to the overly weak immune system.
- They are now undergoing routine diabetes, osteoporosis, cardiovascular diseases, and colon cancer screening. It may appear ordinary, but it is an excellent indicator of their life expectancy and the causes of their deaths, which became very similar to the causes of death in the general population.
- Patients who have no undergoing infections with other bacteria, viruses, or yeast could undergo viral testing for HIV every 6-12 months, a period that was previously much shorter.
- It also included the necessity of screening for other sexually transmitted infections, including gonorrhea, chlamydia, and trichomonas in females.
HAART

To understand how HAART therapy works, we know that viruses are not as independent as bacteria. Neither can they replicate on their own, but rather “enslave” the cells and use their protein-forming machinery to produce new viruses. Viruses live to multiply and multiply to live. Antiviral agents work by disrupting this process of multiplication on various steps, and a combination of several antivirals that act on different stages tend to have the best effect.
HAART regimen consists of a group of different classes of drugs that include:
- Nucleoside reverse transcriptase inhibitors (NRTI): They include drugs as Zidovudine and Lamivudine. They act by inhibiting the enzyme known as reverse transcriptase, which is essential in allowing the viral genetic material to be translated to a “language” that a cell can understand to use its protein-building machinery. Its side effects include a tendency to shift the body’s metabolism from aerobic to anaerobic metabolism, therefore causing lactic acidosis.
- Non–nucleoside reverse transcriptase inhibitors (NNRTI): They include drugs as Nevirapine and Delavirdine. They work by a different mechanism than NRTI, although they eventually achieve the same effect. NRTI acts by competing with viral reverse transcriptase enzyme, while NNRTI acts by binding to the enzyme itself, rendering it non-functional. NNRTI are generally more potent than NRTI.
- Protease Inhibitors: They include drugs as Atazanavir and Darunavir. They act by inhibiting the viral enzyme protease. The protease enzyme helps the viral particles mature by “cleaving” excess amino acids from the final protein product. Without such cleavage of proteins, viral particles become non-functional. Resistance may develop from first-generation protease inhibitors, necessitating the utilization of 2nd generation protease inhibitors as Tipranavir and Lopinavir. Common side effects with protease inhibitors include GIT upset as nausea, vomiting, diarrhea, and metabolic abnormalities such as insulin resistance and dyslipidemia.
- Integrase inhibitors: They include drugs as Bictegravir and Dolutegravir. They act by inhibiting the enzyme responsible for integrating the viral genetic material into the cell’s one. Therefore they stop the operation of viral replication after the reverse transcriptase. Integrase inhibitors are generally well tolerated by patients with few side effects that are mostly confined to GIT side effects.
- Fusion inhibitors: The only drug in use today of this class is Enfuvirtide. They act by inhibiting the virus from attacking the cell in the first place, and therefore they act on the first step of the cycle. They are now quite limited both in production and usage due to the increasing number of discovered antivirals with a better safety profile, better effects, and higher activity against resistant strains.
- Chemokine receptor antagonists (CCR5 inhibitors): They are a new class of drugs approved by the FDA in 2007. The primary drug of this class is Maraviroc. It acts in a similar way to fusion inhibitors.
Previously, CD4 count was a strong determinant of whether a patient should take antiretroviral agents or not, this is no longer the case, and new guidelines suggest that treatment should be initiated regardless of the CD4 count.
Resistance to HIV treatment


One of the causes of the failure of HIV treatment is the development of drug resistance.
There are many mechanisms for resistance, but they all involve a change in the viral genetic material known as mutation.
A virus can easily change its genetic codes and evolve to overcome the body’s defenses and render the identification of the immune system useless.
Resistance is a problem facing many drugs currently in use in the treatment of HIV. Testing for such resistance is, however, possible.
Prophylaxis and treatment of opportunistic infections

Opportunistic infections are caused by organisms that generally don’t infect humans with a competent immune system. They are the most common cause of death in AIDS patients.
Prophylaxis is mainly targeted towards infection with Pneumocystis jiroveci, an organism that causes severe pneumonia. It is initiated when the body’s CD4 count drops below 200 per microliter and is discontinued when it exceeds the number. Trimethoprim-Sulphamoxazole usually serves for prophylaxis.
Prophylaxis against toxoplasmosis is also done if the CD4+ count falls below 100 per microliter. Otherwise, prophylaxis against other infections is not needed.
Treatment of opportunistic infections is essential. They are the leading cause of death in HIV, and therefore their treatment significantly decreased the mortality of AIDS patients. AIDS patients are susceptible to opportunistic infections and aggressive forms of common diseases that affect the average population with milder symptoms.
The most common opportunistic infections associated with HIV include:
–Cryptococcal meningitis
–Toxoplasmosis
-Candidiasis
–PCP
–CMV or Cytomegalovirus
–Herpes Simplex virus
Some of the above conditions may be fatal. Still, most of them are easily preventable through simple protective measures during sexual intercourse and vaccines and prophylactic medications, while others need specific treatment.