

Otitis media which refers to middle ear infection is an inflammation of the epithelium lining the middle ear which is usually caused by infection. The middle ear isn’t easily accessible by pathogens; therefore, its infection shouldn’t be neglected. Otitis media has different routes of infection, however eustachian tube is the most common route followed by a perforated eardrum.
Otitis media is a common disease in pediatric medicine, so mothers are always advised to notice alarming signs of middle ear infection. The incidence rate of otitis media complications is quite low, yet most of these complications are serious and life-threatening.
Otitis media is classified according to its onset into acute and chronic otitis media. Otitis media could be accompanied by accumulation of mucous, pus, or even serous fluid due to overproduction or obstruction of the drainage through the eustachian tube. Inflammatory stages of otitis media could be observed by inspection of the eardrum, for instance, congested red eardrum means active inflammation.
Otitis media is usually presented by the patients as irritability, pain, fever, and impaired hearing. However, in the case of secretory otitis media, the middle ear is filled with non-infected fluid resulting in absence of otitis media manifestations.
Causes & Risk Factors
Otitis media could be caused by different organisms whether bacteria such as streptococci, Haemophilus influenza, Moraxella catarrhalis, and staph aureus, or viruses such as respiratory syncytial viruses, rhinovirus, and adenovirus. A middle ear infection is usually secondary to an underlying infection such as cold, flu, sinusitis, or rhinitis.
The infection could spread through the eustachian tube and reach the middle ear. Moreover, infection of the upper respiratory tract may result in congestion of the mucosa lining the Eustachian tube and subsequently its obstruction. Several risk factors may predispose people to catch middle ear infection such as:
1) Age


Children aging between six months to 3 years are found to be more vulnerable to developing otitis media. Children at this age haven’t developed enough immunity to resist simple infections. Furthermore, their eustachian tube is shorter and less sloping which eases its obstruction and spread of the infection from their upper respiratory tract to the middle ear. Pediatricians believe that three out of every three children aging 3 years have had acute otitis media at some point in their lives.
2) Congestion and Swelling of the Adenoids


Congestion and Swelling of the Adenoids are common signs associated with upper respiratory tract infection. Adenoid is a part of the lymphatic system which traps germs and pathogens and prevents their growth, in case of infection it may show congestion.
People may wonder what this has to do with a middle ear infection. The adenoid is placed beside the opening of the eustachian tube, so if it gets enlarged it may obstruct the eustachian tube, prevent middle ear drainage and increase the risk of otitis media.
3) Eardrum (Tympanic Membrane) Perforation
is surely an alarming sign with multiple consequences, particularly in the case of a middle ear infection. The eardrum is a strong membrane with some flexibility, so it isn’t easily perforated. However, a severe external ear infection may cause necrotizing (damage) of the eardrum. Foreign bodies impacted in the external ear may cause injury to the eardrum, yet eardrum perforation is more common during the trial of an inexperienced individual to extract the impacted foreign body.
The middle ear should be separated from the external ear by the eardrum, so perforation of the eardrum and exposing the middle ear significantly increase the risk of developing otitis media.
4) Allergies


It was found that middle ear infection is more frequent during fall and winter which are the seasons of some seasonal allergies. The exact mechanism of the correlation between allergies and acute otitis media is still arguable. However, the most approved theory is the congestion of the upper respiratory tract associated with allergies may cause over-secretion of mucous and obstruction of the eustachian tube.
5) Immunity Condition


Doctors believe that otitis media is less frequently seen in infants aging less than 6 months because of the passive immunity transferred to them through breastfeeding. Exclusive breastfeeding for babies in their first 6 months reduces the probability of getting a middle ear infection by 13%. Feeding babies with milk formulas or dried milk may increase their suitability for getting otitis media.
Compromised immunity for any reason other than neglecting to breastfeed may increase the risk of getting otitis media. Children with chronic debilitating diseases such as malignancies and uncontrolled diabetes may be more vulnerable to catching any infection, not just otitis media.
6) Poor Air Quality


It is an overlooked risk factor for otitis media. Prolonged exposure to air pollutants such as passive smoking may induce upper and lower respiratory tract inflammation by spreading airborne infections. General immune condition is affected by air pollution, especially in children and elderlies. Patients with a weak immune system are for sure more vulnerable to otitis media.
7) Malnutrition


Unhealthy dietary habits affect indirectly the immune system and increase the vulnerability to infections. A balanced diet covering all the nutrients and vitamins significantly boosts the ability of the immune system to stand against pathogens.
Vitamin A deficiency, as well as obesity, are found as common associations -without clear relation- with a middle ear infection.
8) Improper Management


middle ear infections increase the risk of recurrence and chronicity. Unfortunately, negligence of health issues such as otitis media is usually attributed to low socioeconomic status. Healthcare resources are less available or affordable for many children, especially in developing countries.
Middle Ear Infection Symptoms
Symptoms of otitis media are usually localized and guide the doctor’s attention to the ears. However, many patients could complain of non-specific symptoms such as restless sleep, vomiting, and irritability which will make diagnosing more challenging. Most patients with otitis media complain of the following:
1) Otalgia (Ear Pain)


is the clearest symptom that refers to an otitis media. Children who can express themselves complain of ear pain that increases at night because, at the recombinant position, the fluid drainage through the eustachian tube is easily obstructed.
Ear pain could also be referred to as attacks of headaches. Infants or younger children usually express ear pain by rubbing their ears, crying more than usual, and having trouble sleeping. Mothers should notice early signs of irritability and ear pain in their babies to avoid undesirable complications of otitis media.
2) Fever

is a marked sign associated with a bacterial middle ear infection. Otitis media caused by viral infection is usually accompanied by low-grade fever (less than 38.3 Celsius). High-grade fever may be an alarming sign of severe inflammation or the spreading of bacterial infection through the bloodstream. Otolaryngologists (ENT doctors) believe that 2 out of every 3 children having acute otitis media, get feverish.
3) Trouble Hearing

or inability to precept sounds well is a common complaint for many patients with otitis media. Otitis media is usually unilateral affecting one ear, so the reduction in hearing acuity isn’t often significant. A middle ear infection evokes inflammatory reactions that affect the transmission of sound waves through the middle ear. This hearing impairment is temporary and resolves simultaneously while treating the inflammation.
4) Poor Sleep

Due to discomfort and irritability is a frequent complaint, especially from patients with acute otitis media. Lack of sleep drives patients to be more anxious and ask for immediate relief. Patients who get treated surgically by draining the accumulated fluid in the middle ear, are found to get significantly relieved which leads them to fall asleep deeply afterward.
5) Tinnitus

(Buzzing in the ears) and vertigo (loss of balance) is less commonly reported as symptoms of otitis media.
Diagnosis & Evaluation

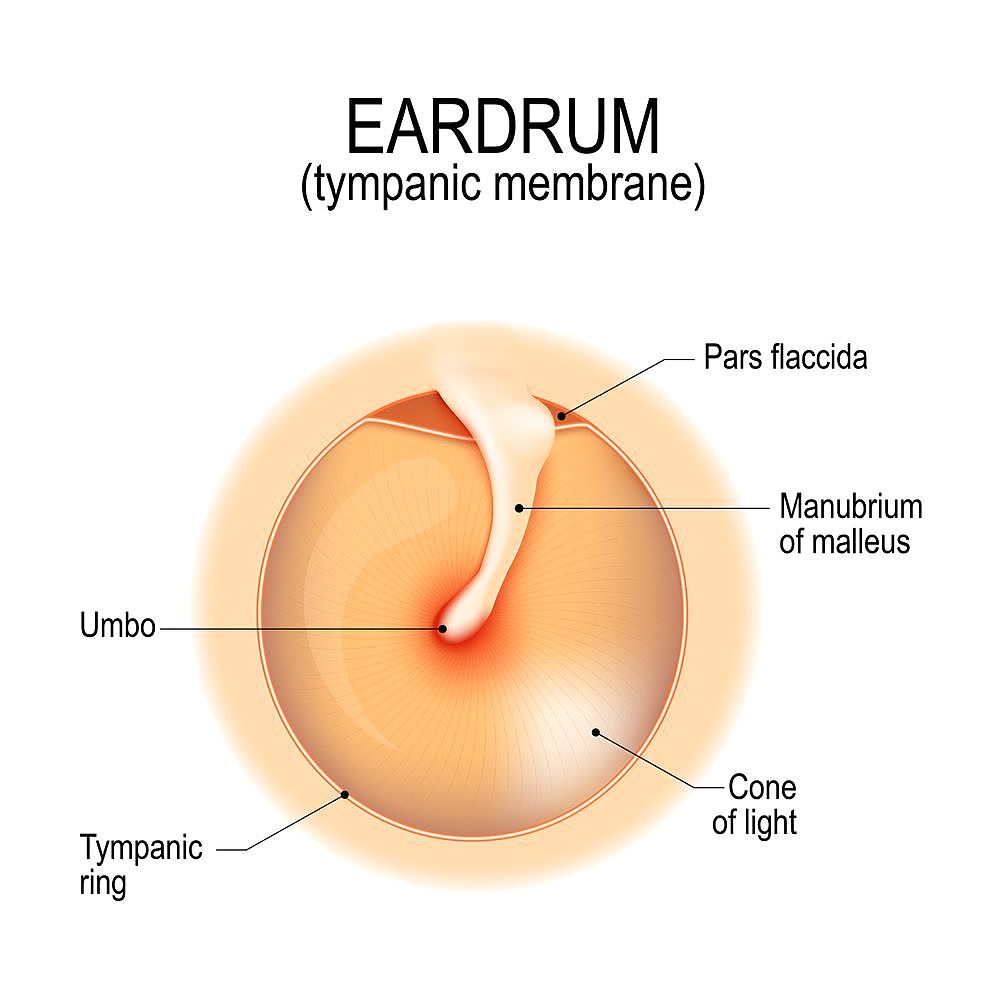
An otolaryngologist will use an otoscope to examine the patient’s ear by inspecting the external surface of the tympanic membrane (ear drum). An otoscope is a hand-sized medical device that has a source of light and a lens to help the doctor have a better look at the external ear and the eardrum.
A healthy eardrum should look like a semi-transparent pearly grey membrane that shows no signs of inflammation or bulging, otherwise, it may reflect an underlying issue in the middle ear. for instance, in acute otitis media, the ear drum is likely to be congested, less mobile, and bulging. The doctor may use a special otoscope called a pneumatic otoscope to confirm the diagnosis of otitis media by assessing the mobility of the eardrum.
For less extent, the following diagnostic modalities are used to diagnose otitis media. Tympanocentesis is a diagnostic and therapeutic procedure in which a small needle is used to puncture the eardrum and drain some fluid that will help the doctor have a more accurate diagnosis. Radiological imaging is not frequently used to diagnose otitis media unless intra-cranial complications such as brain abscess or hematoma (collection of blood outside a blood vessel) are suspected. In such cases, CT or MRI are helpful diagnostic tools.
Laboratory studies and blood tests aren’t used to diagnose a middle ear infection. However, feverish patients may need further investigations such as blood work to evaluate how severely their body is affected by the infection. Hearing tests are used for patients with otitis media only if their doctor suspected significant hearing impairment resulting from the infection.
The clinical findings together with the supportive signs and symptoms listed above are used to reach the diagnosis of otitis media. For almost all patients, there is no need for a lab test or radiological imaging. According to the American Academy of family physicians (AAFP), the diagnostic criteria of acute otitis media include the presence of middle ear effusion (fluid accumulation) showed as less mobile and bulging tympanic membrane (ear drum) in addition to signs and symptoms of acute middle ear inflammation such as erythema of the tympanic membrane and ear pain.
The absence of signs of acute inflammation may indicate chronic otitis media or otitis media with effusion. These criteria are set to guide general practitioners and primary healthcare providers into the right diagnosis, yet it doesn’t replace clinical judgment.
Prognosis


The prognosis (fate) of otitis media varies according to many factors such as the patient’s immunity, the virulence of the organism, and the provided treatment. Most patients with otitis media have an excellent prognosis as they have complete resolution of the infection and gradual restoration of their hearing acuity. Nowadays, the mortality rate of acute middle ear infection is insignificant due to better and more accessible healthcare resources.
Doubtlessly, early diagnosis and treatment result in a more favorable prognosis. Most patients with otitis media show improvement 2 to 3 days after getting treated with antibiotics. Patients with repeated attacks of otitis media may be more challenging to get treated. Complicated otitis media may result in irreversible hearing impairment in the affected ear. moreover, intra-cranial complications of otitis media are serious and life-threatening.
Middle Ear Infection Complications
Fortunately, the incidence of complications resulting from otitis media is almost neglectable. According to AAFP (American academy of family physicians), the incidence rate of otitis media complication is 1 per 100,000 in children and 1 per 300,000 in adults. The risk of complications is much higher for patients who haven’t been diagnosed early, not to mention, uncompliant patients. The complications of a middle ear infection include the following:
1) Perforation of the Tympanic Membrane (Ear Drum)

is a complication of otitis media, yet few doctors may consider it a sign in the course of uncontrolled otitis media. Accumulation of secretions in the middle ear increases its pressure which will eventually cause a rupture of the eardrum. Patients with a perforated eardrum are usually presented with a discharge coming out of the ear other than wax (otorrhea). Patients with otitis media may find transient relief at the time of the perforation followed by persistent ear pain and significant loss of hearing. A perforated eardrum may heal on its own or need suturing according to the extent of the perforation.
2) The Spread of the Infection

is more common in neglected cases of middle ear infection. Atypical causative organisms or resistant strains of bacteria may not respond to therapy and spread in the surrounding tissues. Bacterial infection may reach the mastoid bone behind the ear resulting in acute mastoiditis. Acute mastoiditis appears as a congestive painful swelling over the bony protrusion behind the ear. Chronic otitis media may form fluid cysts or abnormal masses in the middle ear.
In rare cases, the infection spreads from the middle ear to the intracranial tissues such as the meninges covering the brain matter. Inflammation of the meninges (meningitis) is the most common intracranial complication of otitis media followed by brain abscess. Meningitis is a serious condition and should be treated carefully. The frequent signs that may indicate the development of meningitis are neck stiffness, severe headache, and projectile vomiting. Infection may spread to the inner ear causing labyrinthitis that may cause irreversible damage to the neural endings precepting sound waves.
3) Facial Nerve Paralysis

is a potential risk of otitis media. The facial nerve passes through the posterior and medial walls of the middle ear, therefore in patients with otitis media, the inflammatory process may irritate the nerve or cause an accumulation of fluid that compress it against the bony wall. In such a case, the patients complain of loss of facial expression on the side of the affected ear. Complete restoration of the facial expression is believed to occur 2 to 3 weeks after treatment of the underlying cause (otitis media).
Treatment of Middle Ear Infection

Once the diagnosis of acute otitis media is established, the objectives of treatment are to resolve the symptoms, treat the infectious process with antibiotics, and prevent a recurrence. Prescription and administration of Antibiotics are controversial in the treatment of acute otitis media, and recommendations vary by guidelines your healthcare facility follows. It is believed that up to 90% of patients with acute otitis media recover spontaneously within two weeks with just nutritional support and symptomatic treatment, consequently, antibiotics should not be administered to all children at first.
Delaying antibiotic medication in certain patients decreases treatment costs, reduces adverse effects, and limits the emergence of resistant strains of bacteria. The wait-and-see approach approved by the American academies of pediatrics has its guidelines, so it should not be applied to all patients with otitis media. Analgesics such as paracetamol (acetaminophen) and ibuprofen are also prescribed to relieve the pain. Aspirin is less commonly used to reduce pain in children to avoid Reye’s syndrome.
Surgical intervention is indicated in certain scenarios of otitis media. Patients who have acute otitis media with a bulging and congested eardrum that medication failed to relieve after 48 hours are indicated to have a myringotomy. Myringotomy is a surgical procedure in which a small incision (hole) is made in the eardrum to allow fluid accumulating in the middle ear to be drained through the external auditory canal.
The aim of myringotomy other than drainage of fluid or pus from the middle ear is to avoid uncontrolled rupture of the ear drum. In cases of chronic otitis media with effusion, myringotomy could be indicated in addition to the insertion of a ventilation tube to prevent the continuous buildup of fluids in the middle ear.