

Peripheral artery disease is a common circulatory problem of the blood vessels that supply your legs and feet. It happens when there is a narrowing of the arteries of your legs. It decreases the blood flow to your leg muscles, which causes nerve injury and affects other tissues. This problem is a sort of cardiovascular disease because it affects blood vessels.
The build-up of fatty deposits in the walls of the arteries makes them narrower and restricts blood flow to the legs. This condition is called atherosclerosis and represents the most common cause of peripheral vascular disease.
There are two main subtypes of peripheral artery disease: proximal and distal. The proximal type involves the aortoiliac and femoropopliteal sites, and the distal involves the infrapopliteal region. The distal type affects the medial aspect and leads to poorly compressible arteries with high mortality.
You may develop that disease if you are a smoker. Smoking is the most significant risk factor. Also, other risk factors increase put you at a higher risk, such as diabetes mellitus, hypertension, high cholesterol, obesity, and heart or kidney diseases.
Many patients with that disease may be asymptomatic in the early stages, while some patients have leg pain or cramping during walking (claudication). This pain increases by walking and disappears after minutes of rest. The site of pain indicates the narrowed artery location, which is usually in the calf. The severity of claudication differs from mild to severe.
Severe claudication can debilitate you from walking or doing physical activity. The symptoms may also include weakness, numbness, heaviness, coldness, redness, infections, and sores. In the advanced stage, pain may even occur at rest or when you are lying down. Peripheral artery disease has high-risk vascular complications, such as:
- Myocardial infarction
- Stroke
- Renal artery disease
- Mesenteric disease
The peripheral arterial disease affects about 30% of older persons in the general population. The principal symptom, intermittent claudication, occurs in those under 50 years but increases in older individuals.
If you have leg pain during walking or exercise, you should see your doctor as early as possible. Ask your doctor about this disease if you’re 70 years even if you haven’t any symptoms. Seek your doctor’s advice if you have:
- A positive family history of peripheral artery disease, heart problems, or stroke
- Hypertension
- Elevated total cholesterol
- Smoke now or in the past
- Obesity
Diagnosis of Peripheral Artery


Your doctor will rely on some tests and investigations to diagnose your conditions, such as:
- Physical examination to look for signs of peripheral artery disease and check blood flow in your legs and feet. It also helps your doctor listen for a whooshing sound in your leg arteries.
- Ankle-brachial index (ABI), which assess and compare blood pressure between your legs and arms
- Magnetic resonance angiography
- Peripheral angiography, in which your doctor uses a needle to put the dye in your bloodstream then takes an X-ray to determine the blocked arteries.
- Screening for peripheral artery disease
- Screening for peripheral artery disease and correlation to cardiovascular problems with ankle-brachial index
- Doppler ultrasound to check blood flow and determine the blocked arteries and the site of occlusion
- Blood tests to search for risk factors like high cholesterol and diabetes mellitus
The United States Preventive Services Task Force doesn’t recommend routine screening with ankle-brachial indexes because no evidence indicates that early detection leads to a better prognosis.
Peripheral artery disease has high-risk vascular complications, such as:
Myocardial infarction, stroke, renal artery disease, and mesenteric disease
The management of peripheral artery disease depends on its severity. The first step is lifestyle changes by cessation of smoking and regular exercise. Medications include medical treatment of diabetes, hypertension, and high cholesterol. If symptoms persist, surgical intervention is the next step. It includes angioplasty, bypass surgery, or thrombectomy. All procedures keep the blood vessel patent and restore blood flow.
What does cause peripheral artery disease, and what are its risk factors?


The most significant risk factors for peripheral artery disease are smoking and diabetes mellitus. Inflammation and thrombosis, high lipoprotein A and homocysteine levels, and chronic kidney disease increase the risk of peripheral artery disease by 1.5 times. High risky populations include:
-
- People with leg symptoms, exertion, or ischemic rest pain
- People aged 65 years and more
- People between 50 and 69 years old and have a cardiovascular problem
- People with an abnormal lower extremity pulse examination
- People with coronary, carotid, or renal artery disease
- People with a Framingham risk score of 10%–20%
- People with experienced chest pain
1. Family history and old age also have an association with that disease. Peripheral artery disease is associated with coronary heart disease and cerebrovascular disease because both are present in more than half the patients who have peripheral artery disease. Two population studies found that more than 95% of patients have a minimum of one cardiovascular risk factor.
2. Atherosclerosis represents the most common cause of this disease. However, the less common causes include inflammatory disorders of the arterial wall and noninflammatory arteriopathies.
3. Some studies suggested that 50% of all patients are smokers. Heavier smokers develop peripheral artery disease more than light smokers. Also, former smokers have an increased risk compared with never smokers.
4. By the same pattern, poor diabetes control increases the risk of peripheral artery disease. Patients with diabetes may be asymptomatic due to the co-existence of neuropathy in a substantial proportion. 50% of patients with diabetic foot ulcers have peripheral artery disease. Studies conducted in diabetic patients found that the duration of diabetes mellitus, the level of glycemic control assessed by glycated haemoglobin, and the use of insulin are associated with peripheral artery disease.
5. If you have elevated blood pressure, you are at risk for peripheral artery disease. Hypertension is second to current smoking as the most contributive risk factor in the population.
6. Also, dyslipidemia may ride you to the same disease with increased total cholesterol to high-density lipoprotein ratio. Total cholesterol, high-density lipoprotein, and triglycerides are associated with peripheral artery disease.
7. Light-to-moderate alcohol consumption is less consistent for peripheral artery disease. There is no association between alcohol and claudication incidence, but the positive correlation of alcohol consumption with smoking is a significant risk factor for peripheral artery disease.
How much do you know about the symptoms and signs of peripheral artery disease?
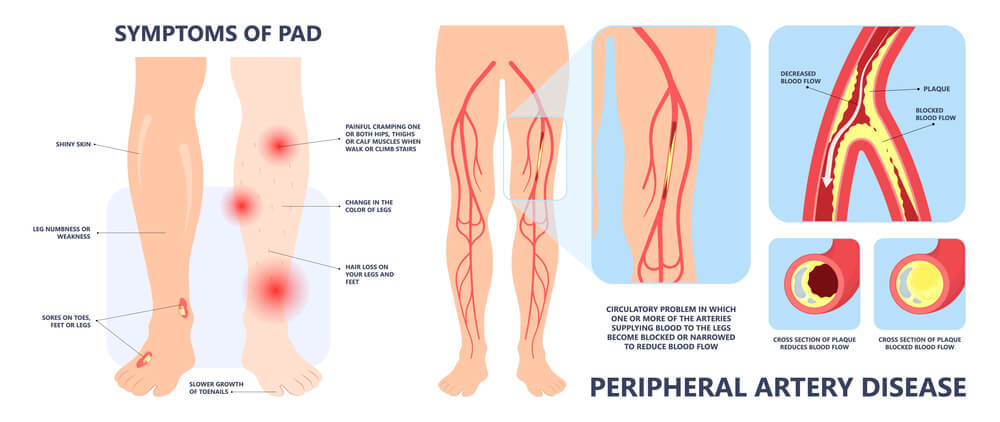

If you have a mild problem, you may have no symptoms, but symptoms appear as the disease progresses. The classic complaint of that disease is intermittent claudication, which means pain in your legs with physical activity. However, up to 4 in 10 patients have no leg pain. This pain is usually in the calf muscles of the affected leg and gets better after rest.
Pain can affect different muscle groups, such as the calf, buttock, pelvis, feet, and thigh. During exercise, muscles need more oxygen. The arteries can increase blood flow, so the oxygen delivery to the exercised leg increases. In peripheral artery disease, the vessels can’t respond appropriately to the oxygen demand by the muscles. As a result, lactic acid accumulates in leg muscles due to anaerobic respiration.
The outward symptoms will not appear until the artery has narrowed by 60% or more. The site of pain indicates the located occlusion. Stenosis or occlusion of the aorta causes bilateral lower limb claudication.
Early symptoms include:
-
- Intermittent claudication (leg discomfort, pain, and cramping) develops with activity, relieves by rest, and comes back when you resume exercise.
- Numbness, weakness, or heaviness in your leg muscles occur during walking or climbing stairs.
Decreased blood flow causes this cyclic pain that relieves after ending exercise because your muscles need less blood flow at rest.
If you don’t control the disease, it progresses, and you will feel severe symptoms which include:
-
- Burning sensation or achiness in your feet and toes during rest, especially at night
- Sores or wounds in your legs or feet that won’t heal
- Coldness and color change in your legs or feet
- Wasting or shrinking of leg muscles
- Hair loss or slow hair growth in your lower limb
- Your toenails grow slowly.
- The skin of your legs becomes shiny, smooth, and thin.
- Weak or absent pulsation in your legs and feet
- Erectile dysfunction
- Pain in your arms when writing or knitting
Critical limb ischemia means one or more ulceration, gangrene, or rest pain in the foot for more than two weeks. There are differential diagnoses in lower limb pain related to exercise. Critical lower limb ischemia is often resistant to opiates analgesia and may be hard to differentiate from neuropathy. Patients hang their legs over the edge of the bed to relieve the pain. Don’t miss acute limb ischemia as delays increase the risk of limb amputation.
How much do you know about this?

You should be aware of the complication of this disease to keep yourself.
Peripheral artery disease is a warning sign because if you have a plaque in your legs, you probably have it in another site, too. It may occur in the arteries of your heart (coronary artery disease).
Also, it may build in your kidney (renal artery disease). You may have it also in the arteries of your brain, leading to a stroke.
If you have the disease and diabetes, you will be at a high risk of critical limb ischemia. The prognosis of this disease in diabetic patients is worse.
Diabetic patients with peripheral artery disease are five times more likely to have an amputation than other patients with that disease.
What about the epidemiology of peripheral artery disease?


Lower limb peripheral artery disease is characterized by occlusion anywhere from the aortoiliac segment to the pedal arteries.
The prevalence of that disease is equal in both men and postmenopausal women, but symptoms are more prominent in men. Black people have a lower ankle-brachial index than whites.
A recent systematic review found that the global prevalence of this disease was 5.6% in 2015. Atherosclerosis of the lower extremities causes cardiovascular morbidity and mortality that affects more than 230 million persons worldwide.
The prevalence in the United States is 7% which equals 8.5 million adults. This estimate depends predominantly on data collected in the 1990s.
How can doctors diagnose your peripheral artery disease?


Your doctor will ask about your medical history and review the risk factors.
Your doctor will look for abnormal findings, which include:
- Weak or no pulsations below the site of artery occlusion
- Muscles wasting and atrophy
- Bluish discoloration of the leg
- Coldness of the affected limb when compared with the other
- Shiny and thin skin and hair loss
- Poor wound healing in the affected area
If your doctor suspected peripheral artery disease, he would use an ankle-brachial index test. It is a non-invasive test that compares the blood pressure in your legs and the blood pressure in your arms at rest and after exercise. If blood pressure readings in the legs are lower than those in the arms, it suspects a blockage in the arteries that deliver blood from the heart to the legs.
If you have leg pain, but your Ankle-brachial index score is average standard, you may need additional tests, such as:
Lower limb Doppler ultrasound helps your doctor evaluate blood flow through your blood vessels and identify the site of occlusion and the extent of atherosclerosis.
Your doctor may do imaging by angiography. The technique is the insertion of a catheter inside your femoral artery and injection of a dye followed by a taken x-ray. Contrast angiography is the most available and used imaging technique. It allows your doctor to treat an occluded vessel at the time of diagnosis.
Computed tomography angiography with x-ray and contrast agent provides direct imaging of the arterial system. This test is helpful in patients with pacemakers or stents.
Magnetic resonance angiography uses a combination of a large magnet, radio frequencies, and a computer to make detailed images of your blood vessels.
Also, blood tests measure the amount of cholesterol and triglycerides in your blood and check for diabetes.
Management of peripheral artery disease!


The main goals in treating these patients are to control the risk of adverse cardiovascular outcomes, enhance functional capacity, and keep limb viability. Multiple coexisting conditions are common in these patients with additional challenges in treatment.
Early diagnosis, lifestyle changes, and treatment can stop the disease progression. Disease symptoms might be reversible if you kept exercise combined with careful management of cholesterol and blood pressure.
A) Lifestyle changes include:
- Stop smoking. Ask your doctor about programs to stop smoking.
- Live healthily. Eat a healthy diet high in fibers and low in cholesterol, fat, and sodium. Avoid trans and saturated fats made with vegetable oils. If you are obese, you should decrease your weight to lower cholesterol and raise your HDL cholesterol.
- A regular exercise program, such as walking, can aid in the treatment. People who walk regularly have a definite improvement in the walking distance before experiencing leg pain.
- Control other health conditions, such as elevated blood pressure, diabetes mellitus, or elevated cholesterol.
- Keep away from stress and do exercise, yoga, or meditation.
- Care of the skin of your feet to reduce infections and decrease the risk of complications.
B) Treatment by medications include:
- Antihypertensive drugs -like angiotensin-converting enzyme inhibitors- decrease your high blood pressure.
- Statin medication lowers your high cholesterol.
- Hypoglycemic drugs lower blood sugar levels.
- Antiplatelet drugs -like aspirin- may reduce the risk of heart attack and stroke.
- Cilostazol helps patients with intermittent claudication exercises longer before they develop leg pain, so it improves your walking distance.
C) Supervised exercise programs:
If you are diseased, you should walk at home for at least 30 to 60 minutes every day. This program includes:
- Walk until the pain reaches a moderate level, then stop.
- Wait until the discomfort ends.
- Walk again.
In severe cases, your doctor should restore the blood flow to decrease pain at rest and improve wound healing.
An angiogram is the first step your doctor should perform to restore blood flow.
D) Endovascular (surgical) procedures include:
- Balloon angioplasty, in which your doctor passes a balloon through a catheter into your arteries. The balloon expands inside your arteries, pushes against the plaques, and widens the lumen inside your arteries.
- Stents are tiny metal support coils that your doctor inserts into your arteries through a small opening using a catheter. Stents expand against the inner wall of the blood vessel to support it and keep it patent.
- Bypass surgery, in which your doctor uses a part of your healthy vein or a synthetic replacement to create a bypass for blood flow around the stenosed area in your leg arteries.
- In Atherectomy, your doctor uses a catheter with a blade at its end to remove plaque.
Finally, you should live healthily and see your doctor when you feel leg pain or discomfort because early detection of the disease leads to a good prognosis.