
Syphilis is the name given to a severe and often life-threatening sexually transmitted disease (or STD). The causative agent is a bacterium called Treponema pallidum, which is capable of colonizing the skin or broken mucous membranes, usually found in the genitalia. This disease is usually transmitted by sexual contact, although there are other causes of infection. Many infected patients ignore that they are infected with syphilis because it has a latent and asymptomatic nature at first, but as you will see in this article, the long-term consequences can be fatal. That is why some governmental institutions include syphilis tests to detect this disease as a requirement before marriage. Similar precaution is taken with pregnant women who receive prenatal care, and there’s a way to prevent the infection from being transmitted to the newborn baby (congenital syphilis) by running a screening test for syphilis.
In syphilis, the leading signs and symptoms should be dived in three main stages of the disease. Studying each of the stages separately will give you enough insight and understanding to be able to identify if something is wrong with you and lead your suspicion.
The stages of syphilis and corresponding symptoms are as follows:
A) First stage (incubation period: 14 to 21 days)
1- A painless sore or ulcer


It is also called “chancre.” It is small and open and typically appears on the genitals or rectum, but they can also be seen in the mouth or skin. Some sores can also be hidden deep in the vagina, in the foreskin, inside the rectum, and in other less visible places. Generally, a chancre heals on its own after 21 to 42 days. They have a firm surface, and they are rounded and painless, but sometimes they are open and moist. Usually, only one sore appears, but some patients may have two or more.
It is easy to mistake a chancre with an incarnated hair, a grain or a harmless protuberance, and since the sores are not painful and can be found in hidden places, it is possible that they go unnoticed. Chancres caused by syphilis are incredibly contagious, and it is easy to transmit the infection to other people during sexual intercourse.
2- Inflammation of the lymph nodes in the area of the sore


As you may know, the lymph nodes are small glands in charge of filtering a clear circulating fluid through the lymphatic system: the lymph. These glands become inflamed in response to infections and tumors. Enlarged lymph nodes are usually located near the area of the sore, usually the groin.
The lymph circulates the body through ducts similar to blood vessels in an alternate circulation called lymphatic system. These small glands store white blood cells, and undergo replication when there’s an infection. That is when lymph nodes start to swell.
B) Second stage (4 to 8 weeks after primary syphilis)
1- Skin rash

This is part of the secondary stage of symptoms. Skin rash is usually located in the palms of the hands and the soles of the feet, but it can also affect other parts of the body. It can last between 2 and 6 weeks per outbreak, and sometimes it is hard to notice because it is not usually itchy and may appear and disappear for a period of up to 2 years.
2- Ulcers


Around 10 to 15% of patients with secondary syphilis start showing dry and superficial erosions in the skin. They have a silver-gray color with a red areola, and can be found in the mucosa of the palate, tongue, pharynx, larynx, gland of the penis, vulva, anal and rectum. These lesions are not pruritic but they are highly infective due to their high content of treponema.
3- Wet, warty patches


They are known as condylomata. Around 10% of patients show high white or gray lesions in warm and humid areas such as the genitals, perianal region, perineum and the intertriginous regions of gluteal folds, nasolabial, armpit, interdigital folds, the feet and under the breasts. These injuries then undergo hypertrophy forming condylomatous plates that appear in the perineum or around the anus.
4- Fever

In secondary syphilis, fever (defined as a temperature higher than 100.94 ° F) usually lasts more than three weeks, and it is pretty much a constant. But in many cases it is found with no additional symptoms and it is difficult to trace the source of the infection. This is named fever or unknown origin (FUO).
Diagnosing a FUO case triggered by syphilis can be quite difficult sometimes, and doctors need to take into account your clinical history and physical examination to obtain essential clues leading to the diagnosis. In this way, doctors avoid an erratic, expensive, and ineffective search, given the large number of possible etiologies (infectious, connective tissue diseases, and neoplasms). Thus, if you want to aid in the diagnosis, answer every question you are asked with the truth, even when it makes you feel embarrassed because it will contribute to a quick and effective diagnosis.
5- General malaise


This symptom, like many other related ones, may disappear within a few weeks or may appear and repeatedly disappear for up to one year. It is a consequence of all the other bothersome sensations that come along with the disease and the metabolic stress your body is going through as your immune system tries to fight the infection.
6- Lack of appetite

As we have previously considered, syphilis has the characteristic of appearing and disappearing without major symptoms. But one that is quite recurrent in patients with this disease (especially in the second phase) is lack of appetite, clinically named anorexia. This can lead to major complications such as malnutrition and thus contribute to impair the already beaten immune system of the patient.
7- Muscle and joint pain


They are found throughout the disease, but in the first stage it is a mild discomfort that is easily attributed to something else. During the second phase of syphilis, muscle and joint pain can become a significant problem and force patients to look for medical help.
8- Swelling of the lymph nodes

The increase in size or consistency of the lymph nodes is called adenopathy or adenomegaly. The ganglion may be enlarged by increasing the number and size of the lymphoid follicles. Adenopathy in the secondary phase of syphilis is a consequence and manifestation of systemic disease.
9- Visual problems


Visual alterations in secondary syphilis are frequent, and there are various types. In many cases, patients have a small and irregular pupil that accommodates for near vision but not before luminous stimuli. This is usually found in the physical exam but not in a day-to-day setting. However, after a few months or years visual problems become more pronounced and may even lead to optical atrophy.
10- Hair loss

The medical term is alopecia, but in this case it is called syphilitic alopecia. This is an uncommon manifestation in patients with syphilis. It only appears in 4% of them. It is associated with skin scaly lesions in the scalp, but may not have any particular lesion associated with the alopecia patches in a type of hair loss called essential syphilitic alopecia.
Essential syphilitic alopecia can be further divided in different clinical patterns. The most common is called “Moth-Eaten” or stubble pattern. It is characterized by the presence of small patchy alopecic plates, which are not entirely hairless. They have an irregular size, poorly-defined edges, non-scarring characteristics, and no inflammatory or peeling signs. The alopecic plaques are located predominantly in the parieto-occipital region, possibly due to a more significant deposit of treponemes or a richer local vascularization. However, it can affect other hairy areas such as the beard, eyelashes, the armpits, the pubis, the trunk, and even the legs.
C) Third stage (Symptoms depend on which organs have been affected)
1- Damage to the heart and blood vessels
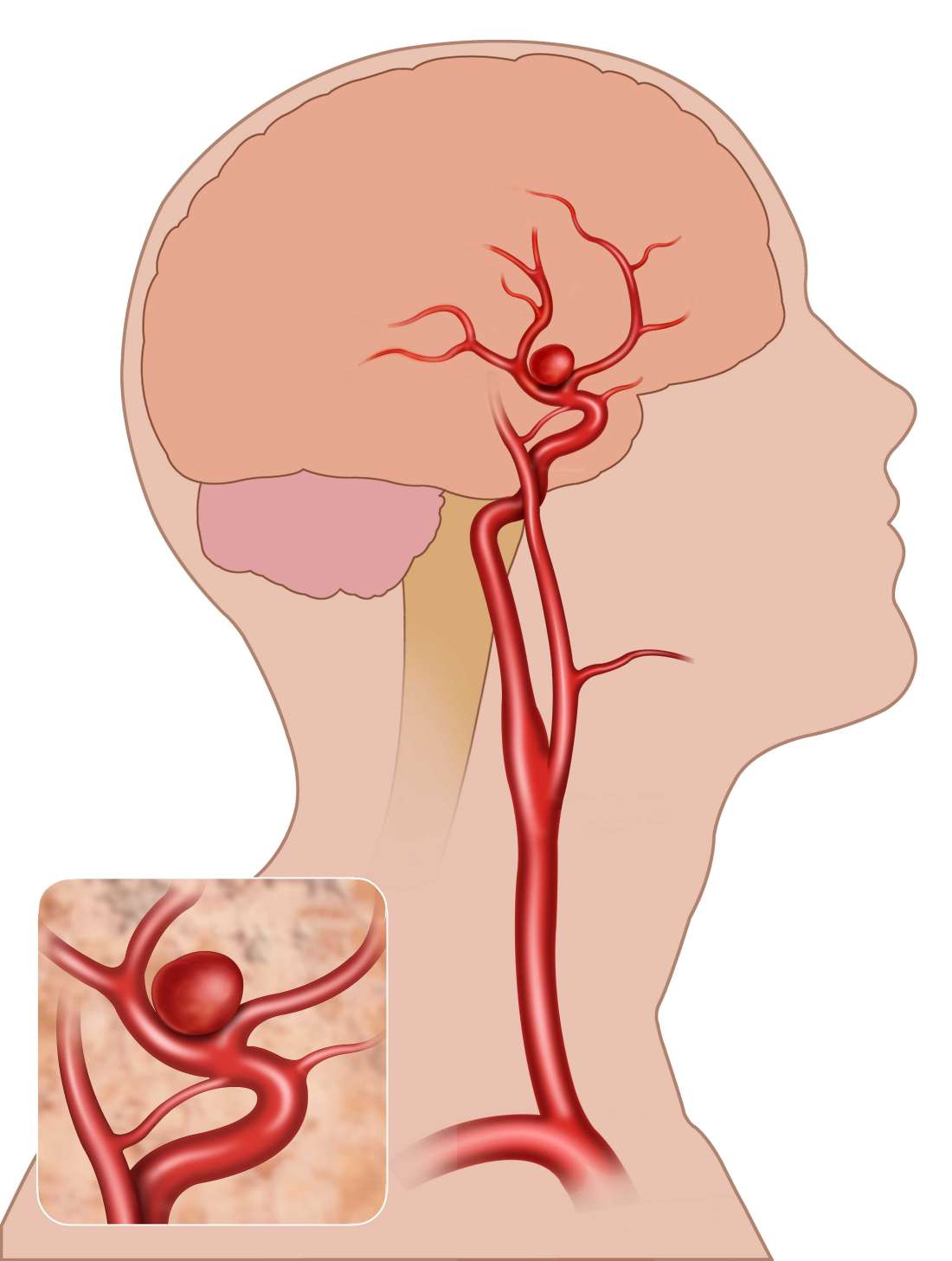

In an advanced stage, syphilis may cause aneurysms or valvular heart disease. They can have an obliterating endarteritis, which affects the vasa vasorum of the aorta and causes middle layer necrosis, a destruction of elastic tissue and subsequent aortitis with aneurysm formation.
This is not the most common symptom, as it is diagnosed in 10% of untreated patients. But it may remain asymptomatic and still affect the patient and increase their risk of cardiovascular event because it is known that 85% of patients with untreated syphilis has certain degree of alteration in the heart or the major blood vessels. However, this complication is not common in patients who are diagnosed and properly treated.
2- Disorders of the central nervous system


In general terms, this is another related disease known as neurosyphilis. It consists of a superposition of parenchymal disturbances in the vascular lining of the meninges. As it is part of the third stage of initial syphilis, it can be asymptomatic at first because patients may not have clinical manifestations but will have brain and spinal fluid abnormalities. These abnormalities include pleocytosis, increased protein, decreased glucose, or positive response in the VDRL test, which makes the lumbar puncture necessary if we want to diagnose this health problem.
Neurosyphilis is the consequence of the damage to the blood vessels of the meninges, brain, spinal cords, etc. The parenchyma is affected as well, and undergoes severe destruction of nerve cells, especially in the cerebral cortex. This area of the brain is in charge or regulating the movement of the body and coordinating cognitive function. Thus, patients with neurosyphilis may experience paresis (weakened movements), aphasia (difficulty to control movement), and many different psychiatric manifestations.
Neurosyphilis is a complication of syphilis that requires a differential diagnosis with others diseases, such as tuberculosis, fungal infections, tumors, subdural hematoma, chronic alcoholism, etc. Given the variable presentation of neurosyphilis, the diagnosis may be difficult, although the demonstration of specific antibodies treponemal in the cerebrospinal fluid helps doctors reach an accurate diagnosis faster.
Tabes dorsalis is yet another damage mainly caused by demyelination of the posterior column, ganglia and dorsal roots. They are typically covered by myelin sheath, a substance that isolates nerve cells just as cables are wrapped by a plastic material. The myelin sheath is important to make the nerve impulse faster, and demyelination in tabes dorsalis leads to poor nerve transmission and many problems, including ataxia, paresthesia (numbness and tingling in the extremities), fecal incontinence, sexual impotence, etc. Cranial nerves may also be affected and the auditory and visual function may be altered at any stage of the disease, especially in the case of congenital syphilis.
3- Tumors of the skin, bones or liver


Late syphilis often features tumors and growths in various parts of the skin, deep in internal organs as in the liver, and the bones as well. They are granulomatous lesions, not painful but visible in imaging tests and often difficult to diagnose when they are located in internal organs and there is no other leading sign or symptom to suspect syphilis. In some cases, these lesions may be surrounded with a local destruction of the tissue, and if you take samples and examine them under the microscope you will be able to see spiraled bacteria called spirochetes that correspond to T. pallidum.
You don’t need to experience all of these signs and symptoms at the same time to suspect syphilis. Two or three of them are enough for a strong suspicion, especially if you’ve had more than one sexual partner for the last months. If this is the case, request an appointment with the health care provider as soon as possible. Be especially careful if you:
- have had intimate contact with a person who is now diagnosed with syphilis or any other sexually-transmitted disease,
- have been involved in high-risk sexual practices, such as having multiple sexual partners, unknown sexual partners or,
- have been using intravenous drugs.
Syphilis can be easily cured with medication if treated early. But without treatment it may lead to serious problems such as brain damage, paralysis, and permanent blindness. The highest risk population are sexually-active young adults, with ages ranging from 20 to 35 years. That is why it is so important to perform STD tests: the sooner you know you have syphilis, the sooner you can get rid of it.
Syphilis treatment

Penicillin is the drug of the choice to treat syphilis, CDC regimens of treatment differ according to the stage of the disease.
1- Primary, secondary and early latent syphilis (less than one year):
The CDC recommends “benzathine penicillin G” single dose intramuscular (2.4 million units).
In the case of penicillin allergy, CDC recommends “doxycycline” twice daily orally (100 mg) for 14 days or “ceftriaxone” once daily intramuscular (1g ) for 10-14 days.
2- Late latent syphilis (more than one year) and syphilis of unknown duration:
The CDC recommends “benzathine penicillin G” 3 doses intramuscularly (2.4 million units each) every week.
In case of penicillin allergy, CDC recommends “doxycycline” twice daily orally (100 mg) for 30 days.
3- Treatment of neurosyphilis:
In this case, the CDC recommends “aqueous benzyl penicillin” intravenously every 4hrs (3-4 million units) or by continuous infusion for 10-14 days. or “procaine penicillin ” single dose intramuscular (2.4 million units) for 10-14 days. plus “probenecid” 4 times daily for 10-14 days (500 mg ) orally.
4- Pregnant females:

A) Primary , secondary and early latent syphilis(less than one year):
The CDC recommends “benzathine penicillin G” single dose
In the case of penicillin allergy, CDC recommends “erythromycin” 4 times daily orally (500 mg) for 14 days or ceftriaxone once daily intramuscular (1g ) for 10-14 days or azithromycin once orally (2g).
Doxycycline is contraindicated in pregnant females, as it crosses the placenta, and thereafter the drug is delivered to the fetus as well.
Erythromycin doesn’t cross the placenta, thus it’s considered a preferred choice in case of penicillin allergy.
B) Late latent syphilis (more than one year) and syphilis of unknown duration:
The CDC recommends “benzathine penicillin G” 3 doses intramuscularly (2.4 million units per each dose) every one week.
In case of penicillin allergy, CDC recommends “erythromycin” 4 times daily orally (500 mg) for 30 days .
Surgical treatment may be required in late stages.
5- Treatment of syphilis in infants:


Syphilis can be transmitted through the placenta in non-treated pregnant females, and the transmission depends on the stage of syphilis, with primary and secondary syphilis carrying a higher risk.
The CDC recommends “aqueous benzyl penicillin” single dose intravenous (100,000-150,000 units/kg/day) for 2 weeks. or “procaine penicillin ” single dose intramuscular (50,000 units/kg/day) for 2 weeks.
These drugs are recommended in infants diagnosed as congenital syphilis at birth based on clinical and laboratory evaluation and investigations, or in the infants who are born to mothers who weren’t adequately treated, even if there is no evidence for infection in infants.
In infants who are born to mothers who are treated adequately and don’t have any evidence of infection, follow up is recommended for them.
Some advices should be put in consideration


Penicillin shouldn’t be taken orally or in combination, as the usage of two types of penicillin is absolutely contraindicated.
In patients who are diagnosed with HIV associated with syphilis, no additional drugs are needed, but the duration of therapy becomes longer and the follow-up is mandatory.
In the treatment of late syphilis, the interval between the doses is acceptable up to 14 days, but if the pregnant woman missed the dose, the course of treatment should be restarted again.
Benzathine penicillin is preferred to procaine penicillin in the treatment of syphilis in adults, and aqueous benzyl penicillin is preferred to procaine penicillin in the treatment of syphilis in infants.
Procaine has side effects, such as gastrointestinal tract upsets, but it’s well tolerated by the patient. Some patients complain of hallucinations and psychological changes, while others complain of fever and convulsions. These side effects are well tolerated and need no treatment. Only severe cases only may require treatment.
Doxycycline is preferred as a second line for treatment (not in the pregnant females) if desensitization is not available. Desensitization is a procedure that aims at decreasing penicillin allergy by administering small doses of penicillin in the hospital orally or intravenously for 4-12 hour. Thereafter, patients can respond well to penicillin treatment as penicillin is preferred as a first line for treatment.
Desensitization is important in the case of pregnancy, neurosyphilis, late syphilis, and congenital syphilis.
The goal of treatment is to eradicate Treponema pallidum and this effect is responsible for a type of reaction called Jarisch-Herxheimer reaction.
Jarisch-Herxheimer reaction is caused by releasing inflammatory mediators by the immune system as a response to the dying treponema pallidum organism. It occurs within 24 hours after receiving therapy. The patient displays a rash, fever, myalgia, headache and tachycardia. It doesn’t have a special treatment. The patient just needs supportive therapy as antipyretics and analgesics.
In pregnant females, this reaction can lead to early labor, but this side effect should be prevented at the initiation of therapy.
Follow-up

Reinfection can occur after the treatment of syphilis, so follow-up is required. Patients with early syphilis should be tested after 6 months and one year, and patients with latent syphilis should be tested after 6 months, one year and two years. Also, patients with HIV and syphilis should be tested after 3 months, 6 months, 9 months and one year. In the case of patients who didn’t receive penicillin as a first for treatment should be tested after 3 months, 6 months, 9 months and one year.
Patients with late syphilis should be tested for life, while patients with neurosyphilis should be tested each 6 months for 3 years. Pregnant females should routinely be tested for syphilis at the beginning of the infection, and pregnant females with syphilis should be tested each month until delivery.
Pregnant females who had fetal death after 20 weeks should be tested for syphilis. In high-risk communities, pregnant females should be tested once in the third trimester and once at delivery.
Homosexual individuals should be tested repeatedly, as reinfection is common among them. Patients with neurosyphilis should be tested for HIV as well.
Prevention of syphilis

Condoms are an effective method to prevent the spread of the organism, but the surest way to prevent the transmission is by holding a a mutually monogamous relationship with a sex partner.
Abstaining for sexual acts can also reduce the risk of infection. The sex partner should receive preventive treatment, one dose of benzathine penicillin G (2.4 million units) is recommended intramuscular when the sexual act was less than 3 months even if the results of the investigations were negative during early stages of the disease. If more than 3 months have passed since the sexual encounter during early stages of the disease, treatment should be received according to the results of the investigations.
Circumcision doesn’t prevent syphilis infection, although it can prevent HIV.
Sharing needles between drug addicts can help to spread the infection, thus, drug addicts should use a new needle and stop sharing needles.