We usually link malignancies and cancer with hard lesions and tumors. That’s why it is sometimes difficult to talk clearly about certain blood cancer types. Multiple myeloma is one of them, and even though it was described initially in 1848, it represents nowadays close to 10% of all types of blood cancer.
What is multiple myeloma?


Multiple myeloma is a cell malignancy we can find in the human blood. There are many types of blood cancer, depending on the type of blood cell involved in each case. In multiple myeloma, we have an abundance of monoclonal plasma cells. These are white blood cells, commonly known as B cells. In normal circumstances, these cells create antibodies (immunoglobulins) and contribute to fighting disease. They are essential for both viral and bacterial infections.
However, in multiple myeloma, plasma cells’ overabundance takes excessive space and resources, displacing other cell lines and reducing their numbers. The disease is also associated with bone tissue destruction and elevated levels of monoclonal paraprotein. This is an abnormal immunoglobulin produced by defective plasma cells.
Before multiple myeloma, we usually have another premalignant condition known as monoclonal gammopathy of undetermined significance. Doctors often address this condition as MGUS. During this time, plasma cells go through overlapping mutations. They change the way plasma cells divide and their capacity to proliferate. As they do so, plasma cells start taking 10% of the bone marrow or more, and paraprotein values begin to rise.
Inflammation in the bone marrow apparently has a vital role in causing multiple myeloma. Certain inflammatory substances called cytokines are the ones that promote the growth of abnormal cells. After they turn into cancer, multiple myeloma affects the blood and several organs as well, including the bone tissue, the kidneys, and the nervous system.
Multiple myeloma symptoms
The signs and symptoms of multiple myeloma depend on various factors. Some cases can be asymptomatic; others can be very severe. Having symptoms or not depends on the course of the disease and the severity of the abnormality.
The most common symptoms include:
1. Bone pain


Despite being a blood-related problem, bone pain is one of the most important symptoms. Multiple myeloma causes bone pain in up to 70% of patients at the time of the diagnosis. The most commonly affected area is the lumbar spine, but others may be involved as well. In some cases, bone pain is not accurately felt or reported, but the doctor finds bony tenderness or pain without tenderness upon examination.
2. Pathologic fractures


What differentiates pathologic fractures is the force required to produce them. Since the bone tissue is severely affected by multiple myeloma, it becomes weakened and more susceptible to fractures. These fractures are prevalent, and they can be severe or very mild (as in smaller bone lesions). However, they are always revealed in an X-ray in 93% of patients, and they are naturally more common in the lower extremities. Pain is more common when pathologic fractures involve 50% of the diameter of the bone. In smaller fractures, dull pain or bony tenderness is more common.
3. Compression of the spinal cord


The spinal cord requires strength and flexibility of the bony structures and the joints to function correctly. In multiple myeloma, these structures are compromised, and the resulting compression causes numerous symptoms in the lower extremities, such as numbness, weakness, and tingling. This is also another cause of back pain, often located at the lumbar spine. However, spinal compression may occur at more than one site and sometimes warrants physicians’ careful investigation.
4. Bleeding

Multiple myeloma is a proliferation of plasma cells. But they take the space and the resources of other cell lines, reducing their numbers. Bleeding occurs when platelets are severely reduced as a complication of multiple myeloma. In some cases, it is the monoclonal protein that inhibits the action of clotting factors, too. So, we can have bleeding with or without thrombocytopenia.
5. High levels of blood calcium


There’s consequent destruction of bone tissue and calcium release to the blood. Such a high level is usually a very dangerous sign in other solid tumors. However, it only triggers nausea, thirst, constipation, muscle cramps, drowsiness, and sometimes confusion in multiple myeloma. In some cases, it also leads to amyloidosis, which is thoroughly described below.
6. An increase in infection rate


It may seem paradoxical that we are having high levels of immune cells and an expansion of the infection rate at the same time. However, these plasma cells do not work as they should, and sometimes displace other white blood cell lines that are also important to defend the organism against infectious agents. That’s why many multiple myeloma patients have pneumococcal infections, herpes zoster, or infections with Haemophilus bacteria. Having more frequent infections may appear a minor problem, but it is actually one of the leading causes of death in multiple myeloma patients. We should be especially careful when applying chemotherapy because the risk of infection is even higher during the first 2-3 months.
7. Higher viscosity of the blood


As mentioned, there’s an overproduction of plasma cells by the bone marrow. Thus, there is also an increase in the number of cells in the blood and its viscosity. Symptoms of hyperviscosity usually appear after it is 4 times greater than usual. In these cases, patients start feeling general malaise, mental fogs, headaches, drowsiness, and other physical symptoms such as fever, hazy vision, bruising, and tingling in the skin. As the disease advances, and in susceptible patients, we can also have a higher risk of stroke and heart attacks. Higher viscosity of the blood is also a cause of papilledema, seizures, and hemorrhage in the retina.
8. Neurologic problems

Multiple myeloma is associated with several neurologic symptoms and syndromes. One of the most important is carpal tunnel syndrome, which has a higher incidence in multiple myeloma patients than the average. This is because there’s excessive deposition of amyloid proteins in the carpal tunnel. These patients are also more susceptible to bacterial meningitis, usually due to a meningococcal or pneumococcal infection. These are typically late-stage problems, and their onset depends on how fast the disease is diagnosed and how accurate the treatment is.
9. Anemia

We mentioned the displacement of other cell lines due to the proliferation of plasma cells, and that’s why these patients suffer from anemia. Their red blood cell levels drop dramatically, causing weakness, sluggishness, malaise, and other symptoms. In these cases, the patient also looks pale and tired during physical examination.
10. Visual problems

Some patients with multiple myeloma may also have severe visual problems, including a retinal hemorrhage or a macular detachment. As such, their vision may be severely affected or not, depending on the stage and progression of the disease.
11. Soft-tissue masses in the skin


Sometimes, doctors can find small masses in the skin after a close inspection. In multiple myeloma patients, these masses are probably an accumulation of plasma cells, and they can be found almost anywhere in the body. Those found in the skin are easier to notice. Still, we can also have them in the ear canal, the eye, the rectum, prostate, gastric mucosa, or the abdomen’s inner covering of the abdomen (peritoneum).
12. Organ enlargement


Several organs in multiple myeloma patients become enlarged, especially the liver and the spleen. Both organs are essential to clear the blood from toxins, defective cells, and other abnormalities. But even if they try to even out the excess of plasma cells, they cannot bring back their numbers to normal. Another organ that is usually enlarged is the heart, which is known as cardiomegaly. This is because there’s a deposition of immunoglobulin in the heart tissue, which triggers an increase in the organ’s size.


13. Amyloidosis
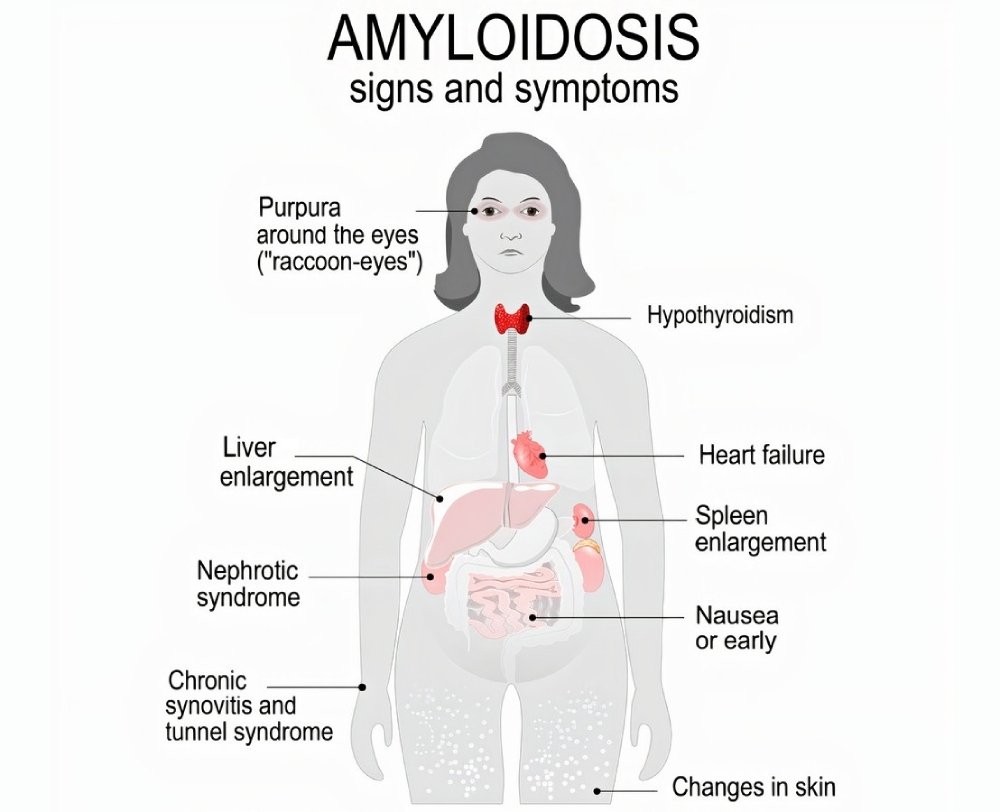

Similar to the carpal tunnel, other areas of the body can undergo amyloid deposition. In patients with amyloidosis, we will have additional symptoms, such as macroglossia, skin lesions, swelling of the shoulder joints, and dark circles around the eyes. The deposition of amyloid can explain these symptoms in the shoulder joint, the tongue, waxy nodules in the skin, or the capillaries and small blood vessels.
14. Kidney problems

Late-stage multiple myeloma causes renal failure or renal insufficiency. These problems affect 25% of patients with this type of hematological cancer, and it is more common in patients with amyloidosis and high levels of calcium in the blood.
As noted, multiple myeloma has a variety of signs and symptoms. However, around 30% of cases are discovered by merely running a routine blood test. One-third of the patients are diagnosed when they have a bone fracture and other complications.
Diagnostic protocols and tests (multiple myeloma diagnosis)


Since most cases are found incidentally, it is essential to rule out several diseases before making a final assumption. In the diagnostic considerations of multiple myeloma, we should also think about similar problems, such as a primary lymphoma of the bone, or a metastatic bone disease, which also have pathologic fractures and behaves similarly in many cases. We should also rule out Waldenstrom macroglobulinemia, a lymphoproliferative disorder that also affects B lymphocytes. Still, instead of monoclonal paraprotein, we have a very high level of immunoglobulin M, also known as macroglobulin.
After suspecting a case of multiple myeloma, most patients require several studies to evaluate what type of blood cancer it is and how far it has reached to compromise the patient’s health.
The most important exams in the workup include:
Blood tests
They are naturally part of the workup, and many patients are actually diagnosed after a routine blood test. Complete Blood Counts are important to evaluate the number of blood cells, which is typically depleted. Coagulation is also abnormal, and the erythrocyte sedimentation rate is generally increased.
Urine collection
It is sometimes vital for the diagnosis and should be evaluated in a 24-hour collection. That’s the only way to accurately quantification a substance called Bence Jones protein, as well as creatinine and protein clearance. Having a very high protein level in the urine (higher than 1 gram in 24-hour urine) can help diagnose the disease.
Electrophoresis
This study can be useful to determine the presence of Bence Jones proteins in the urine. It also detects M proteins in the blood, and serum concentrations of 30 g/L and higher are important for diagnosing multiple myeloma.
Immunoglobulin levels
Multiple myeloma may feature suppression of specific immunoglobulins. Thus, detecting immunoglobulin levels is important to diagnose the disease.
C-reactive protein and Beta-2 microglobulin
C-reactive protein reflects very well the activity of interleukin-6, a substance that promotes growth in plasma cells. Beta-2 globulin levels can be used as a tumor marker, and it is also increased in renal insufficiency.
Serum viscosity
This measurement is particularly important in patients with epistaxis (nosebleeds) and those who have been found with very high levels of M protein.
X-rays
Using radiography is very helpful to find pathological fractures and other lesions in the bones. It is an integral part of the differential diagnosis because we should always rule out metastasis to the bones. Plain radiography is often enough to make a diagnosis. Still, we should perform a complete series of X-rays to cover the entire body and evaluate the presence of small pathological fractures and bone degradation areas (lytic lesions).
Magnetic Resonance Imaging
This imaging technique is advantageous to evaluate spinal cord compression and lumbar lesions in the spine. It detects abnormalities in asymptomatic patients with apparently regular X-rays, so it is imperative in the workup.
Positron Emission Tomography
It is potentially useful in combination with MRI to evaluate the patient and provide more accurate follow-ups. However, it is not yet a part of the standard practice in multiple myeloma.
Biopsies and aspiration
This is an important test for diagnosing multiple myeloma because the disease is characterized by an increase in the proportion of plasma cells in the bone marrow. Bone aspiration is also useful, but not as accurate as a biopsy.
Cytogenetic analysis of the bone marrow
It offers a prognosis of multiple myeloma because it shows which genes are compromised. A deletion of 17p13 is so far the most severe abnormality associated with a higher risk and shorter survival.
Histologic examination
In blood histological studies, we will find giant plasma cells, which are up to 3 times larger than usual. They have particular characteristics that contribute to the diagnosis.
After testing the patient and performing a physical exam, we can make an accurate conclusion by using multiple myeloma diagnostic criteria. These criteria are divided into two groups:
- I: Plasma cell accumulation in soft tissues, examined by biopsy
- II: More than 30% of plasma cells in the bone marrow
- III: Spikes in monoclonal globulin measures (IgG greater than 3.5 g/dL or IgA greater than 2 g/dL)
- A: 10-30% of plasma cells in the bone marrow
- B: Spikes of monoclonal globulin, but lower than the above
- C: Bone degradation and lesions
- D: Residual levels of IgG (less than 600 mg/dL), IgM (less than 50 mg/dL) or IgA (less than 100 mg/dL)
Using the above criteria, we can diagnose multiple myeloma when we have:
- B, C, or D plus I or II
- A, C, or D plus III
- A, B, and C
- A, B, and D
We also have two staging systems to evaluate and stratify the patient according to the severity of the disease. They are the Salmon-Durie staging system and the International staging system, which was revised in 2015.
Multiple myeloma treatment (treatment options)


Multiple myeloma is a complex disease with a difficult treatment, and there are many limitations in the current therapeutic protocols. When treating a patient with multiple myeloma, the goal of therapy is to obtain the best possible result in the first try. When this is the case, the patient’s survival rate improves considerably. However, it requires a complete understanding of the natural history of the disease and choosing the best treatment for each patient and their phase of the disease.
Treatment is focused on slowing down the disease process and treating the complications associated with multiple myeloma. We need to remember that multiple myeloma is incurable, but proper treatment and specific modalities offer the best results. There is even a slight chance of cure and complete disappearance of M protein in the blood, which only happens in 3% of the cases. Some treatment protocols are instrumental, but they can cause severe side effects, including new malignancies.
Most patients with multiple myeloma undergo chemotherapy as a part of their induction therapy, which is the first phase of the treatment followed by maintenance therapy. But there are many other options and procedures. In short, these are the leading methods to treat multiple myeloma:
Chemotherapy and immunotherapy
Chemotherapy is required for all patients with symptomatic multiple myeloma, but not in asymptomatic cases. As chemotherapy and immunotherapy are applied, it is essential to measure the M protein, which helps doctors evaluate if the treatment is doing as it should. The goal is to achieve a reduction of 50% in M protein levels.
The type and intensity of chemo and radiotherapy depend on whether or not the patient is eligible for a transplant. So, it is broken down into three categories: young and healthy patients who can be transplanted, high-risk patients who can be transplanted, and elderly patients who cannot be transplanted.
A 4-day regime is often chosen in young and healthy patients, including intravenous vincristine, doxorubicin, and dexamethasone. This therapy is also known as VAD, and it is followed by 4 days of oral dexamethasone. Other regimens also use lenalidomide, thalidomide, bortezomib, or daratumumab.
In high-risk patients who are candidates for transplant, novel agents are commonly used instead of VAD therapy. These patients have a very high tendency of relapse and need lenalidomide, thalidomide, or bortezomib as a part of their treatment, followed by stem cell transplantation.
Finally, elderly patients who are not candidates for transplants typically use melphalan and prednisone for 4 days, repeated every 4-6 weeks for one year. However, there are many other regimes with combinations of dexamethasone with daratumumab, bortezomib, lenalidomide, or cyclophosphamide, depending on each case.
Radiotherapy
Radiation therapy may also be used, but mainly to reduce the risk of fracture and treat the spinal cord’s compression. It is only used if the bone pain is mild, and if 50% or a lower proportion of the bone is compromised by multiple myeloma.
Transplantation
It is usually performed with bone marrow from the same patient or stem cells from the patient’s peripheral blood. Doctors harvest stem cells from the patient and irradiate the whole body to destroy the bone marrow’s defective bone marrow. This is followed by a reinfusion of the stem cells or bone marrow. Only a few patients may receive bone marrow from someone else, but it is not the standard procedure, and several tests should be performed, except for twin donors.
Interferon-alpha therapy
According to recent research, interferon-alpha can be used to prolong remission in high-risk patients. In other words, it delays the reappearance of multiple myeloma when the chance of such an event is very high.
Bone and skeletal therapy
Besides radiation therapy, we can also use other substances to promote skeletal health and reduce fractures’ risk. For example, bisphosphonates are useful to inhibit the activity of osteoclasts.
Therapeutic options for other complications
Depending on the complications and the symptoms of each patient, a set of drugs and therapeutic options can be used. For example, erythropoietin in anemia, pins to stabilize pathologic fractures, corticosteroids, and spinal cord compression surgery.
References
Kumar, S. K., Callander, N. S., Alsina, M., Atanackovic, D., Biermann, J. S., Castillo, J., … & Godby, K. (2018). NCCN guidelines insights: multiple myeloma, version 3.2018. Journal of the National Comprehensive Cancer Network, 16(1), 11-20.
Abramson, H. N. (2018). The multiple myeloma drug pipeline—2018: A review of small molecules and their therapeutic targets. Clinical Lymphoma Myeloma and Leukemia, 18(9), 611-627.
Albagoush, S. A., & Azevedo, A. M. (2018). Cancer, Multiple Myeloma.
Ramakrishnan, N., & Jialal, I. (2019). Bence-Jones Protein. In StatPearls [Internet]. StatPearls Publishing.