

When angina is mentioned, the classical picture that comes to mind is a chronic, slowly debilitating condition related to fat plaques clogging the arteries and causing a gradual obstruction. This idea is not wrong in most cases; however, a particular type of angina is very different from this, and is called Prinzmetal’s or Variant angina. Dr. Myron Prinzmetal first discovered it as a syndrome featuring chest pain found in a patient who can tolerate usual physical exercise. On the other hand, he had a chest pain that is “triggered” usually early in the morning.
Why does it happen?
Unlike stable angina, the heart’s blood vessels’ caliber, “the coronaries,” is typical in between attacks. The pathology here is that the smooth muscles of the blood vessels walls reversibly contract, narrowing the blood vessels’ diameter suddenly and causing a marked decrease of blood flow, thereby inducing pain.
You should also know that this doesn’t mean that the coronary arteries are always in a state of relaxation. Instead, they are in a state of continuous, yet varying degrees of contraction finely tuned according to the body’s condition and needs. Any imbalance of the various chemical substances controlling such process induces spasm. When the spasm occurs, it varies from a mild spasm, in which pain can only be produced if the heart is exerted enough that the supply no longer matches the demand, to a severe spasm that may cut off the blood supply entirely from a part of the heart, leading to a heart attack -also known as myocardial infarction-. The provoking factors for these spasms are various, and although they are still not largely known, some known factors include:
-
- Tobacco smoking
- Hyperventilation
- Cocaine use
- Drugs as amphetamines
- Alcohol
- Cold exposure
Although the presence of coronary spasms doesn’t mean that the coronary artery itself is atherosclerotic, the presence of both types of angina is possible. The only known common risk factor between the two types is smoking, and cessation of smoking can prevent and potentially help treat both types. To summarize the main difference between stable angina and Prinzmetal’s, we can say that while stable angina is a demand problem, Prinzmetal’s angina is a supply problem.
Symptoms of prinzmetal’s angina

The main difference between stable/unstable angina and Prinzmetal’s in symptoms is the timing and the presence or absence of exertion. Prinzmetal’s angina is mainly characterized by:
♦ It usually occurs at midnight or early morning.
♦ Although it may also be precipitated by emotional stress, it is unrelated to physical exercise.
♦ It may develop several hours after alcohol intake, a feature unique to this type.
♦ Since the main pathology of variant angina is the spasm of arteries, other diseases that involve the same pathology are commonly found in such patients. The most prime example is Reynaud’s disease, a disorder where your fingers’ blood vessels constrict, causing their whitish, then bluish discoloration and pain, along with migraine headache, where its mechanism essentially involves constriction of blood vessels of the brain. Both diseases have a higher prevalence among women, and thus Prinzmetal’s is more common in females.
Diagnosis of prinzmetal’s angina


The main challenge in diagnosing Prinzmetal’s angina is differentiating it from conditions displaying similar symptoms. Several methods can achieve this:
- A comprehensive medical history of the patient, and especially a description of the patient’s symptoms and how they develop, when they occur, and whether they are associated with effort or not.
- To differentiate it from unstable angina, however, would need additional tools and investigations. The primary studies used for the diagnosis of vasospastic angina include:
- Lab studies as serum levels of lipids to help exclude atherosclerosis of the coronary arteries.
- Cardiac enzymes, since they are released when cardiac muscle cells die, is a good indicator of the degree of deprivation of the heart from blood -also known as ischemia-.
- Since chest pain has various causes, traditional cardiac imaging as a transthoracic echocardiogram can help exclude other common causes of chest pain related to the heart as pericarditis, which is the inflammation of the heart’s covering- and aortic aneurysm or dissection -changes in the wall of the aorta-.
- Electrocardiography, which is a measurement of electrical activity across the heart. In vasospastic angina, a particular pattern of electrical abnormality is noticed when the electrical signal passes across the ventricles. However, this is not seen in between attacks, and thus not very useful in the diagnosis if it is done in an outpatient clinic. To solve this, an ambulatory ECG is used where the ECG electrodes are attached to the body for a day or more to record the event when it occurs.
- Angiography may also be used. It is an imaging technique that is directed towards the blood vessels of the heart. It can demonstrate whether the coronaries are atherosclerotic or not and visualize the site of spasm. It can also be used in provocative tests, where certain substances as ergonovine -a fungal alkaloid- are injected intravenously to detect whether they cause spasm of coronary arteries or not. This type of tests tries to simulate how susceptible are arteries to spasm.
Treatment of prinzmetal’s angina


Vasospastic angina is a cardiac condition, and treatment shouldn’t only focus on the spasm but also on overall cardiac health. In many patients with Prinzmetal’s angina, atherosclerosis is coexistent and should be managed as well through lifestyle measures as physical exercise and diet in addition to the pharmacologic treatment through antiplatelets, statins, and anticoagulants. If atherosclerosis is absent, however, such pharmacologic therapy is unnecessary.
Targeted therapy towards vasospasm includes:
1) Pharmacologic therapy
Pharmacologic therapy aims to relax the vessel wall’s smooth muscles in the short term and prevent the recurrence of their spasm. For short term relief, nitrates are the drugs of choice. Sublingual or intravenous nitrates act within a few minutes, and their effect is outstanding. For long term prevention or “prophylaxis” against attacks, drugs include either long-acting nitrates or calcium channel blockers.
Calcium channel blockers as amlodipine are commonly used as they have a long duration of action. They act by blocking calcium channel, preventing its influx into the muscle fibers, and since calcium is essential for the contraction of muscles, this causes relaxation of the vessel walls.
2) Invasive measures

Most cases of Prinzmetal’s angina improve on medical therapy alone. Still, in a minority of cases, the frequency of attacks remains high even with maximal medical treatment, and in such cases, more invasive measures become a must. Options for treatment here include revascularization using either percutaneous or surgical methods:
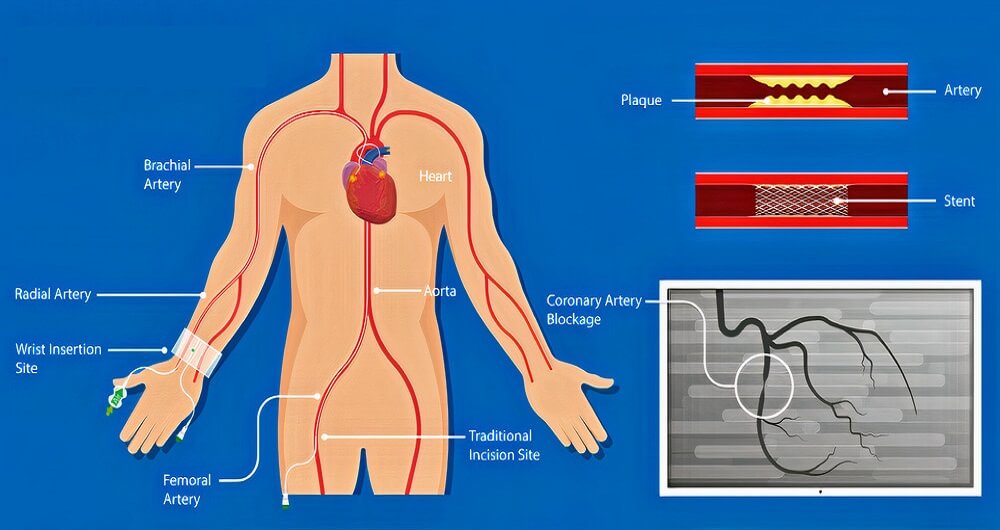
A. Percutaneous intervention:
Percutaneous means through the skin. Such a procedure is usually done by your cardiologist, which involves inserting a “stent” into the lumen of your coronary artery. This is done through a catheter, a tube-like malleable structure inserted into your femoral blood vessels, and goes up your bloodstream to your heart then the coronaries. Such a stent will support your artery’s walls in the event of spasm and prevent their collapse.
B. Bypass surgery:
The above therapy options cover most patients, and surgery for vasospastic angina became rare. It is done on an individual basis and isn’t considered routine. This surgery involves two steps; the first one is creating a “bridge” across the spastic segment of the coronary artery using a blood vessel from the body -as the saphenous veins from the calves-. The same surgery is done in the case of atherosclerotic angina, but here it is less successful, and the spasm may persist. Therefore, the second step is called a “plexectomy” or “denervation,” which cuts some of the nerve supply to the coronary arteries preventing the arteries from going into spasm. You can compare this to an electric motor that keeps producing a noise that won’t just stop, so the best option is to cut off some of the electricity feeding it to slow it down a bit.